Hypermobility Spectrum Disorders

After much ado and chomping at the bit, the brand new 2017 International EDS Classification scheme is out since March 15th, 2017, including the brand spanking newly invented diagnostic category called:
Hypermobility Spectrum Disorders
In addition to identifying 7 new rare types of the now pluralized Ehlers-Danlos Syndromes for a total of 13 recognized as of March 2017, the International Hypermobile Working Group hatched this entire new diagnostic category of Hypermobility Spectrum Disorders as the catch-all bin for all of those who show signs of a connective tissue disorder involving varying degrees of hypermobility, but not enough to meet the new criteria for the still most common yet now “rare” again hypermobile form of EDS aka “hEDS” now.
Nor show any signs of any of the more rare forms of EDS, or any other similar heritable connective tissue disorders. (E.g. Marfan Syndrome, Loeys-Dietz Syndrome, Stickler Syndrome, Osteogenesis Imperfecta, etc.)
In other words, you are bendy to some degree (maybe even a lot), but either not very symptomatic or not in the right ways. Or, if you have signs and symptoms of a CTD but have ruled all other possibilities out (see diagnostic flowchart below), you don’t tick enough boxes or bend enough for a diagnosis of hEDS now since March 2017. Many may be related to bendier people or people diagnosed with a form of EDS.
That is, it is a diagnosis of exclusion of all other possible connective tissue diseases and disorders involving hypermobility of any amount or type:
| 1a – Do they seem like they have some kind of CTD? | 1b – Gather as much medical history as you can to see |
| 2a – Rule out all rare forms of EDS with genetic markers (12 of 13 as of 2024) | 2b – There are 12 types with markers per the 2017 nosology here |
| 3a – If negative by testing for those, then rule out all other possible similar CTDs like: | 3b – Marfans, Loeys-Dietz, Stickler Syndrome, Osteogenesis Imperfecta, Charcot-Marie Tooth |
| 4a – If negative for those, then rule out hEDS | 4b – No genetic test yet*, see hEDS Diagnostic Checklist |
| 5a – If negative for hEDS, then diagnose a form of Hypermobility Spectrum Disorder | 5b – This is a diagnosis of exclusion of ALL THE above! |
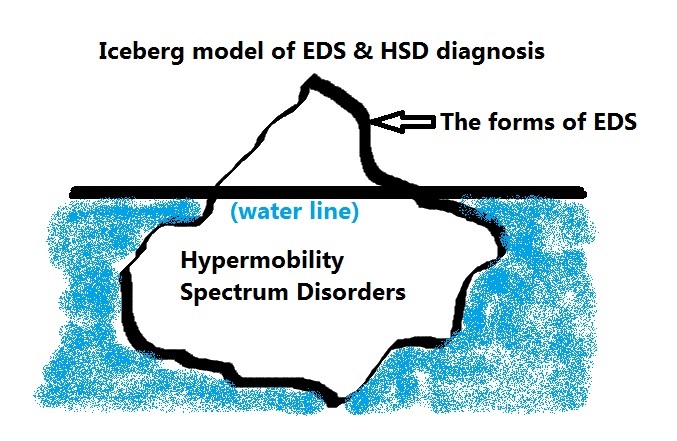
I personally suspect many who are diagnosed with fibromyalgia at this time, but I’m not a doctor. If the forms of EDS are the tip of the iceberg, easly visible above the water, the forms of HSD are like the bulk of the iceberg lurking beneath the water line. Very real, but just much less “visible” to the diagnostic eye – until now, hopefully.
And, as with hEDS, we have not been able to finger a single genetic mutation or SNP to blame for this new category yet. (Nor even a group of same.) And, please note that the newly tightened hEDS criteria, and these new forms of Hypermobility Spectrum Disorders now obsolete and supplant the older terms and diagnoses of HMS, JHS and BJHS.
Edited to add Nov 1, 2024: science has just uncovered a potential new biomarker for people with either hEDS or a form of HSD which could potentially aid in diagnosis in the future. Yes, exciting! But the study needs to be broadened, replicated and then the test brought to market, so try to hold your horses. /End edit
That is, Hypermobility Syndrome (HMS), Joint Hypermobility Syndrome (JHS), and my favorite, Benign Joint Hypermobility Syndrome (BJHS). There was nothing ever very benign about about this latter (nor hEDS formerly “EDS III”) aside from not being lethal, which was the point of that misleading and invalidating term.
I.e, these latter have been “folded into” the newly recognized hypermobility spectrum including hEDS and HSDs now, going forward. I’m not sure how they plan to handle pre-existing diagnoses but check with The Ehlers-Danlos Society.
So, like IBS, it is a diagnosis of exclusion once all other likely causes are ruled out, but the patient still shows signs of hypermobility of varying degrees, with or without symptoms. Some people are just bendy with no apparent issues. The could just be related to someone with a form of connective tissue disease that lends to this.
Yet others like myself, have so stiffened with early onset arthritis and age (despite being extremely bendy prior), that we no longer meet the newly tightened age and sex specific Beighton 9 pt hypermobility scale cut off for hEDS or any other form, but we suffer loads with plenty of disabling and even sometimes life threatening issues just the same after ruling out all other likely CTDs.
And some patients, like leading rheumatologist Dr. Jaime Bravo in Chile told me himself in an email in 2012, “are never lax, I know, I’m one of them.” Boom! So don’t discount yourself or anyone else if you don’t seem to be very or at all bendy.

Look at the whole patient picture and family history, okay? “If you can’t connect the issues… think connective tissues” to quote some anonymous genius. (Not Dr. Heidi Collins, she was quoting them too.)
Need to be Re-Diagnosed?
HOWEVER, The Ehlers-Danlos Society have tried (keyword!) to make it abundantly clear that no one who has previously been diagnosed with the hypermobile form of the Ehlers-Danlos Syndrome(s) has to give up their diagnosis – yet!
The only reason anyone might be re-evaluated or should, is if they were to try to enter into any form of research for hypermobile type EDS, in which case the new, universally accepted (or at least rolled-out) criteria will be applied. Unless a doctor arbitrarily decides to simply reject a prior diagnosis, which is on the doctor, not the patient.
Yes, I’ve heard a couple of early horror stories of this happening already in some places, and patient complaints being wrongly discarded or dismissed – please think twice before doing this please, doctors and nurses!
As I’ve been telling people in my support groups, it’s much like what happened to our dear 9th planet Pluto back in 2006 when we re-classified it to a “dwarf planet” from a “full” planet prior: Pluto did not change a spot or stop orbiting one iota! It’s still the same exact heavenly body and planetoid neighbor we’ve always known and loved.
We humans simply changed our minds about its classification. Like Pluto, I still hurt (orbit) and struggle (and suffer!) just as much or more as I did before right? I didn’t change a spot. I still need and deserve all of the medical attention and support I did previously, regardless of the name you wish to give my condition.
To be clear, I have NOT been re-diagnosed, nor need to be unless I try to join a research project, and then my final diagnosis still remains to be seen at that time. So I do still technically have hEDS yet. But… I’m just trying to be a bit pedantic and calm some of the anxiety “out there” I’ve seen erupt since these new criteria came out.
Further, I’m even seeing a little benefit emerge, as the support group leader for my regional (highly comorbid) MCAD group. Where everyone had been dismissing my suspicions of EDS in them before, as they felt they were not “bendy enough”, now they are giving the new HSD category some real consideration to my relief: mastocytosis and MCAS do NOT cause bursitis and chondromalacia patella, hernias, prolapses, loose teeth and tendinitis, TYVM! (Update 2019: or so I thought. May rethink this in time…)
In fact, here’s a chart I adapted from the last page of this document from The Ehlers-Danlos Society showing the “spectrum” in a table. It roughly ranges from the mildest to the most symptomatic top to bottom, bendy or not:
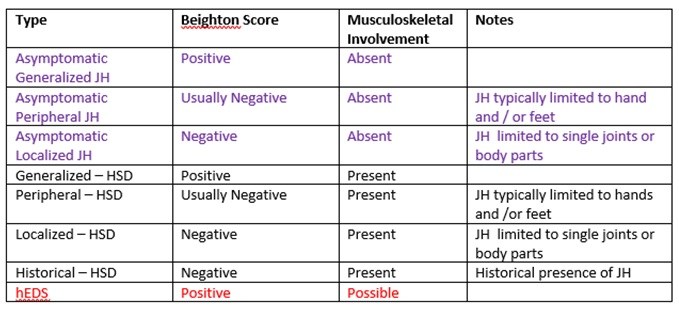
Image ID: A table showing 8 rows of 4 cells each, with a header row titled: Type, Beighton Score, Musculoskeletal Involvement and lastly Notes. The 8 rows beneath each read (left to right):
- Asymptomatic Generalized JH, Positive, Absent, (blank)
- Asymptomatic Peripheral JH, Usually Negative, Absent, JH typically limited to hands or feet
- Asymptomatic Localized JH, Negative, Absent, JH limited to single joints or body parts
- Generalized- HSD, Positive, Present, (blank)
- Peripheral – HSD, Usually Negative, Present, JH typically limited to hands and/or feet
- Localized – HSD, Negative, Present, JH limited to single joints or body parts
- Historical – HSD, Negative, Present, Historical presence of JH
- hEDS, Positive, Possible, (blank)
As you can see, both the top three, (in purple) asymptomatic and next three (in black text) symptomatic forms come in 3 “flavors”:
- Generalized Joint Hypermobility (you “pass” with a high Beighton hypermobility Score)
- Peripheral Joint Hypermobility (it’s typically limited to hands and/or feet)
- Localized Joint Hypermobility (it’s limited to single joints or body parts)
Then the symptomatic forms aka “disorders” listed toward the bottom have one additional “flavor” called “Historical“, indicating that someone may once have been quite bendy, in a generalized way (like myself) but is no longer, but are still symptomatic with musculoskeletal complaints. Followed by lastly, hEDS itself.
Historical-HSD is what I think I would most likely fit now if I were to be re-evaluated as I’m no longer bendy enough to pass the age and sex-specific Beighton score for hEDS now.
But again, much like dear Pluto, I haven’t changed a thing – I’ve simply aged in place, and stiffened with age and early onset spinal and other arthritis. Plus my muscles are very tight from 50 years of holding my very loose skelly together thanks to my loose ligaments and tendons all these years.
I wish to make it abundantly clear as The Ehlers-Danlos Society have tried to also, that the 4 forms of Hypermobility Spectrum Disorders (just above hEDS at the bottom of the chart above) are not necessarily any better or worse than hEDS. They just do not meet the newly narrowed hypermobile criteria for hEDS. I am definitely more symptomatic than many even with hEDS now, even per the newly tightened criteria.
And, hopefully it’s clear that some people (at the top of the list) are apparently just bendy, but don’t seem to have any issues, or at least not yet, smile. (If ever, lucky dogs.)
But others who are only a little bendy or unstable in just a few joints (e.g. just knees, or just hands and feet, or one weak ankle for instance) but have many other symptoms characteristic of a connective tissue disorder (e.g. FGID, IBS, hernias, prolapses, fallen arches, weak teeth, myopia, more) will now be considered for a diagnosis of a Hypermobility Spectrum Disorder.
How Do You Treat HSD or EDS?
If anything, it looks like I “caught” hEDS in 2012 (when I finally was diagnosed), only to “cure” or “lose” it in 2017. Obviously we know it’s not contagious and this is not possible, but I trust you see my point? It’s all a matter of semantics. As The EDS say:
“HSD, just like hEDS, can have significant effects on our health. Whatever the problems that arise, whatever the diagnosis, it is important that these effects are managed appropriately and that each person is treated as an individual. HSD and hEDS can be equal in severity, but more importantly, both need similar management, validation, and care.”
And while there’s technically no cure for any of the forms of EDS nor the newly recognized forms of the new HSD category, there is supportive treatment and preventative measures you can take to avoid needless or excessive injury and prolong your joint health as I’m slowly proving along with a handful of others.
We’re finding various nutritional therapies and custom PT and body work and movement to be most beneficial. Yes, basically “diet and exercise” but with a lot of customization! So it’s worth knowing this is also something you’re dealing with in my opinion, to minimize your pain levels (pain is a mast cell trigger too), and stay as well as possible.
That said, treating our many comorbidities (co-occurring conditions) can also go a LONG way to improving our quality of life. (MCAS, POTS and other dysautonomia, more.)
I hope this has helped to clarify when to suspect and diagnose the new category of Hypermobility Spectrum Disorders a bit. This is new for ALL of us in 2017, so please be patient with everyone, doctors and fellow patients and support group leaders as we all work to wrap our arms and brains around this new diagnosis. I am hopeful that it will allow even more people to receive much needed pain and other support and management instead of just being dismissed for not meeting any other criteria.
As I said on Facebook where I started a new Oh TWIST Hypermobility Spectrum Disorders “Pool”, come on in, the water is fine! Last updated November 2, 2024