When to suspect Ehlers-Danlos Syndrome (EDS)
 I’ll repeat that if you haven’t yet read my About EDS post, please do so now to help make this post more understandable. It is seriously hard to do this topic justice in just one blog post. (Why I’m trying hard to write more off line, smile). Remember the six blind men and the elephant story? EDS is more like 60 blind men and the same elephant. Podiatrist, dentist, neurologist, cardiologist, allergist… the specialist list goes on! (We end up being medical “frequent flyers” alas, despite our best efforts to the contrary). So I’m only sharing a few ways to suspect it. There are almost unlimited symptoms ultimately, since being systemic it affects virtually every body system to some degree and in often unexpected ways. But we have to start somewhere, and this is my start. Others are welcome to do the same. And, not being a doctor, I can’t and don’t expect anyone to take me half as seriously as they probably should, if at all in some cases, thanks to all the misinformation and misunderstanding around this lousy connective tissue disorder. But if I can raise just one other person’s suspicions or “zebra-dar” if you will, much less a doctor’s along the way, I will have succeeded in my mission to bring a small shred of enlightenment to the medical world and hopefully reduce the time to diagnosis and related unnecessary suffering for a few of my fellow sufferers out there.
I’ll repeat that if you haven’t yet read my About EDS post, please do so now to help make this post more understandable. It is seriously hard to do this topic justice in just one blog post. (Why I’m trying hard to write more off line, smile). Remember the six blind men and the elephant story? EDS is more like 60 blind men and the same elephant. Podiatrist, dentist, neurologist, cardiologist, allergist… the specialist list goes on! (We end up being medical “frequent flyers” alas, despite our best efforts to the contrary). So I’m only sharing a few ways to suspect it. There are almost unlimited symptoms ultimately, since being systemic it affects virtually every body system to some degree and in often unexpected ways. But we have to start somewhere, and this is my start. Others are welcome to do the same. And, not being a doctor, I can’t and don’t expect anyone to take me half as seriously as they probably should, if at all in some cases, thanks to all the misinformation and misunderstanding around this lousy connective tissue disorder. But if I can raise just one other person’s suspicions or “zebra-dar” if you will, much less a doctor’s along the way, I will have succeeded in my mission to bring a small shred of enlightenment to the medical world and hopefully reduce the time to diagnosis and related unnecessary suffering for a few of my fellow sufferers out there.
That said, I am not a doctor, so do not take what I write as either gospel, nor as medical advice – let me be clear, you should always consult your preferred medical care provider about your own indvidual health. And… I personally recommend ultimately seeing a knowledgeable medical geneticist if you do suspect any form of EDS, as it strongly resembles several other heritable disorders of connective tissue (HDCT’s) including Marfan’s Syndrome, Osteogensis Imperfecta (OI), and Stickler’s Syndrome, which should be properly ruled in or out. (We have a lot of overlapping signs and symptoms and issues). A medical geneticist will know how to differentiate these. As well as know when to suspect the more dangerous forms of EDS like Vascular (formerly Type IV) or Kyphoscoliotic. (More on that in a later post). And you need to be sure of which “zebra” (semi-rare condition) you are treating for the sake of not only your health, but that of any children you’ve hatched or plan to. Many of these disorders are only finally diagnosed when someone has a child who is much more afflicted than themselves, and the parent only gets diagnosed by proxy. (We’re a surprisingly stubborn bunch in regards to our own health – and often refuse to acknowledge how much pain we’re in until it’s “too late”. I know my late parents sure did). I’ll lastly add that I find many hypermobile people seem to be attracted to one another – I have other theories I’ll share on that in a later post. (I now suspect both of my late parents in hindsight, though it’s most clear on my dad’s side). Something about birds of a feather… (wait, zebras don’t have feathers!)
But I digress. When to suspect EDS? Again… the problem here is I will run out of time to share all the possible ways in a blog post. So, I’ll highlight some of my personal unprofessional theories, again, emphasizing to take what I write with a grain of salt. (Literally, for some of you with POTS, smile). That said, this post IS based on over two years of my personal online observation of literally over 6000 afflicted indviduals with every variation on the theme you can imagine from all over the world via Facebook and the EDNF’s support forum Inspire (http://www.inspire.com) where we all…. (drum roll please), COMPLAIN of all our issues! That is to say, while I’m not a doctor, and am not trying to be, I “see” thousands more “patients” than any doctor ever could without joining me on Facebook and Inspire (and real life), albeit socially. And no, I’m not reporting things I’ve only seen just once or twice, but common themes I see frequently now. (You’ve already read about the biggy, Mast Cell Activation Disorders in my last post – if not, go back and read up!) Why we win this freakish bad health lottery I do not know, but we seriously do. (It is a systemic condition after all). I seriously feel like Alice down the rabbit hole as mentioned in prior posts as I discover more daily, even two years out since falling down my own “rabbit hole”. And much of this is not in the current literature even yet. (Why I’m blogging along with so many others!)
My “Fibro Theory”
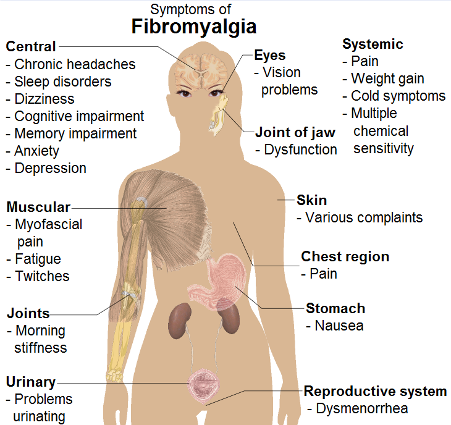 First and foremost, as all my friends and family know well now, I personally believe ALL people with “fibromyalgia” likely have some form of EDS, most likely HEDS. Seriously. I really well and truly now believe that fibro is really just likely a lighter, usually “un-triggered” case of Hypermobile EDS (aka HEDS) based on all the complaints and descriptions I read from thousands of very vocal fibro patients on Facebook and Twitter. (And they’re a very vocal bunch as they struggle to be believed as I once did.) I personally experienced “fibro” since my 20’s (in the 1990’s) that I was not able to eliminate or improve while adhering to a modern working lifestyle all these years, and so just “sucked up” and carried on despite it as best I could. (Not always successfully). Further, all of the remedies fibro patients are finding to help alleviate their symptoms (including careful physical therapy, especially warm water therapy and nutritional work) are exactly what help EDS patients the most!
First and foremost, as all my friends and family know well now, I personally believe ALL people with “fibromyalgia” likely have some form of EDS, most likely HEDS. Seriously. I really well and truly now believe that fibro is really just likely a lighter, usually “un-triggered” case of Hypermobile EDS (aka HEDS) based on all the complaints and descriptions I read from thousands of very vocal fibro patients on Facebook and Twitter. (And they’re a very vocal bunch as they struggle to be believed as I once did.) I personally experienced “fibro” since my 20’s (in the 1990’s) that I was not able to eliminate or improve while adhering to a modern working lifestyle all these years, and so just “sucked up” and carried on despite it as best I could. (Not always successfully). Further, all of the remedies fibro patients are finding to help alleviate their symptoms (including careful physical therapy, especially warm water therapy and nutritional work) are exactly what help EDS patients the most!
Now either that’s one heck of a coincidence, or we’re on to something here. And, again, I’m not a doctor, BUT, I’ve personally yet to meet a fibro patient in real life who does not pass the brightonslide2013 (NOT just the Beighton 9 pt Hypermobility SCALE which is just PART OF the Brighton Diagnostic Criteria in a plot to confuse, sigh) for Hypermobile EDS (aka JHS, HMS, etc.). You could say we got “bright” in Brighton, England, and improved upon Professor Peter Beighton’s brilliant epidemimological field test for hypermobility which was never meant to diagnose EDS, and which misses a large percentage – some say up to 50% – of older EDS patients due to the misguided hyper-focus on the joints only. I can’t agree more with Dr. Jaime Bravo, a leading rheumatologist in Chile with whome I’ve corresponded who posits that Fibromyalgia is just a form of pain experienced by HEDS patients in his “When To Suspect” document he shared with me in 2012. He’s still using the older naming system, so it is called Joint Hypermobility Syndrome on his site here: http://www.reumatologia-dr-bravo.cl . However he also agrees that all these other forms called JHS, HMS etc. should all likely be called EDS III (aka HEDS), now too.
I seriously struggle to silently watch while thousands of fibro patients struggle to control their logically wide-spread pain that isn’t aided by anti-inflammatories or pain meds, or not much, and describe experiences as bad and sometimes worse than my own with HEDS. (Some are also wheelchair bound like I was in 2012. From muscle and fascial tissue pain or a nerve disorder?? I don’t think so!) As one who experienced it up until my “storm” made my “fibromyalgia” feel like a cake-walk, I’d say it makes a lot of sense if you have a slightly loose skelly, but haven’t fully disclocated anything yet. (And no, thankfully few of you will ever have such a bad “storm” or “cascade” of EDS symptom onset, so please don’t needlessly worry, just be aware of your body’s symptoms at all times. That experience is blessedly rare). It seems to me that if all your connective tissues, muslces and fascia are struggling to hold your bones in place, they would naturally be prone to tender points or trigger points (either or both IMHO. Remember the six blind men and the elephant story).
Let’s put this another way. I’ll say I strongly suspect ANY fibromyalgia patient who also has a history of family medical problems on one or both sides, especially including joint pain with or without arthritis (we’re prone to early onset arthritis of all kinds, including OA and RA both), varicose or spider veins, IBS, and any kind of mood or sensory processing disorders. (Hold that thought!) Of course there’s no easy remedy, because those nerve endings that Lyrica is supposed to be addressing are constantly being re-activated as your fascia and muscles are warped and stretched beyond normal range. Toss in our extreme difficulty falling and staying asleep from commonly experienced hyperadrenergia (ultimate cause unknown, but it’s extremely common in the community), and boom: fibromyalgia. Dr. Andrew Holman even posits that anyone who is caused to remain sleepless will develop fibromyalgia in this video here, sort of putting the lie to my theory, smile.)
That said, several of my colleagues and I regularly run into resistance even from the Fibromyalgia community to this notion, they seem to have fought so hard for their current diagnosis, they are highly resistant to any other, even in the face of extreme evident hypermobility viewed in person. (Again, every one I’ve met in real life since 2012 has passed the Brighton Diagnostic Criteria for HEDS, but I’m not a doctor). And as stated in elsewhere, I find narcissism and autism spectrum disorders so common with this condition (my own dad was extremely stubborn and smart, as am I, no surprise), that this doesn’t surprise me. I suspect both many patients and medical practitioners are likely high functioning subclinical autistics (plenty of IQ, not so much “EQ”, or emotional intelligence, lots of black and white thinking) and as such, are extremely prone to jumping to conclusions and not considering any other input or information even in the face of mounting evidence that they should. Everyone, medical practitioners and patients alike needs to be more dialectic, and allow for other possibilities, even if you don’t initially agree with them. You may well be right, but… at least you won’t steam-roll anyone in the process of proving so as is wont to happen with many of us. And I say this fully applying same to myself – you are perfectly welcome to disagree with me on any of these view points as they are just that – opinions. Don’t take me too seriously – nay, don’t take ANYBODY too seriously! Ever! This is just my personal, unprofessional opinion. (Clearly begging for some official statistical backing of some kind some day. Can you tell I’m expecting plenty of blow-back from this one, smile? Reminder, it’s just a personal “theory”. I’m happy to be proven wrong with good statistical evidence.)
Dysautonomia and wonky (usually low) blood pressure

I’ve also yet to meet an EDS patient (zebra) who DOESN’T have some form of dysautonomia, most commonly Raynaud’s phenomenon, low blood pressure (though can sometimes spike or stay quite high), GI motility issues, poor temperature control etc. While a majority will tend to run low blood pressure, some will have the hyperadrenergic variant, and some can run quite high and struggle to stay down. Though one tell-tale sign of MCAD for me is anyone with high (or normal) BP who can get it to suddenly drop a lot (say 30 points or more) by eating known triggers. (One friend literally controls herWhen To Suspect high BP via oatmeal and bananas and chocolate – not a bad “prescription” if you ask me!) We can have any variation on this theme, including NMH, hyperadrenergic or HyperPOTS, etc. that you can imagine. Many experience syncope (fainting) and pre-syncope (dizzyness, light-headedness upon standing too quickly) from low blood volume and poor circulation. Others impinge their vagus nerves and throw up easily, or experience other GI dysmotility. Some can no longer fly in airplanes. Again, combine any of these with chronic pain, IBS, varicose or spider veins, hypermobility and any joint problems, and I strongly suspect you.
Sleeping disorders
I also suspect anyone who has sleeping problems ranging from the aforementioned trouble falling and staying asleep due to hyper-adrenergia (we often get a “second wind” around 9 pm that can keep you well up until 2 a.m.), to all forms of sleep apnea no matter how light or heavy the patient. (Toss in high pain levels, and we’re seriously doomed to be sleepless, sigh). Even thin EDS patients can have obstructive airway apnea from weak laryngeal tissues and tracheas, and lots of variations on a theme of dysautonomia as already mentioned, including Central Nervous System Apnea, sometimes requiring a form of breathing “pace-maker”. I literally had trouble remembering to breathe even in the daytime through my “storm” of 2012 – I only now know the term for this problem in yet again, 20/20 hindsight thanks to some fellow support group members. I suspect this was a by-product of some cranial-cervical settling that I’ve since overcome through nutrional work and re-strengthening, (thank God! I’m not sure all can.) Toss in any form of Mast Cell Activation Disorder (MCAD, wither Mastocytosis or MCAS) and allergies leaving us prone to waking from the cyclical histamine shed around 3 a.m. and no wonder we struggle with sleep! I’ve stopped waking since cleaning up my diet (going allergy and trigger-free) and taking some chlorpheniramine maleate at night (an old-school sedating anti-histamine that doesn’t leave me hung over). That said, I’ve met patients who are literally allergic to some anti-histamines, and others to the dyes and or fillers in a tablet or capsule, so you have to find what works for you in concert with your doctor. (I strongly urge seeing a naturopathic doctor if able). We are literally the most sensitive patients you can find to just about everything, with some common themes around salicylates and gluten sensitivity if not outright celiac disease. So no formulary will work for all! Meanwhile, call me Sleepless in Portland!
But I digresss again. Anyway, combine poor sleep with low blood pressure, chronic pain and joint problems of any kind, and I’m willing to bet dark chocolate I have a zebra on my hands.
Arthritis and auto-immune patients
I also suspect anyone who has early onset osteo-arthritis and any forms of auto-immune disorders, but especially ankylosing spondylitis (my dad and 2 aunts had this, and I have the factor for it) or multiple sclerosis. Don’t ask me why, but I’m now finding that much like with fibromyalgia, a large number of MS patients I meet in real life also show tell-tale signs of hypermobility and joint problems, and lots of food and drug sensitivities. Who knows why this is, but based on my learning from The Mastocytosis Society Conference in 2012, I presonally suspect a lot of MS is secondary due to demyelination from either (common) B12 or other nutrional deficiency issues, or mast cell actviation disorders (or both!), since mast cells are known to “line” nerve fibers, if memory serves. (I’ll double check this, but feel free to let me know otherwise sooner, if you know accurately). I personally think that all the systemic inflammation we experience from either likely leaky gut syndrome, or just plain food allergies (got IBS?) and sensitivities or MCAD of any kind may lead to this. Again, I have no medical basis for saying this, it’s just my hunch and I welcome further exploration. But Dr. Diana Driscoll (fellow EDS patient and therapeutic optometrist) has been positing much the same theory on her great website for years now too. Along with the good folks at http://www.mastcellaware.com.
IBS
Speaking of Irritable Bowel Syndrome, aka IBS, I also suspect most with it, as they likely have either high allergy levels, or some form of MCAD or both (like myself) as do most EDS patients. (Almost all EDS patients react badly to anesthetics, both from over-sensitivity, and over-processing – i.e, we need way higher levels of the “caines” – Novocaine, Lidocaine etc. – to feel any effect, and often get sick from general anesthesia, even days after an operation.) I really don’t think there’s any such thing as “just” IBS. I think it’s all some variation on the afore-mentioned themes of food allergies and sensitivities, and combined with some proclivity to dysmotility from impinged vagus nerves lending to some people’s high nausea rates, so I personally suspect anyone with IBS too. Especially if they also have fibro, natch, which a majority seem to have also! And especially if they have any form of diffuse joint pain or repeated joint problems or hypermobility. (Sensing a theme I hope).
Chronic Pain sufferers of all kinds
One of the most tragic and detrimental misunderstandings EDS patients face is being accused of being drug-seekers due to our chronic and often severe connective tissue, joint and muscle pain from so many micro-tears, subluxations and insults. (We also bruise easily, fwiw). We can suffer from any and all forms of arthritis, neuropathy, neuralgias, radiculopathies, CRPS or RSD and fibromyalgia. Alas, we look good “on paper” or scan, if you will, so doctors and nurses will often wrongly conclude we are just simply drug-seeking based on failure to see any gross joint or tendon displacements or tears, and sometimes even with them! Most minor subluxations will not show up on X-ray, and sometimes not even on MRI or CT even with contrast (to which many of us are allergic!) But let me tell you from experience they sure hurt like the dickens! Thus begins the cycle of doctor-shopping in order to find any practitioner willing to treat our very legitimate complaints and chronic pain, leading to patients often having a long “history” of discarded doctors behind them in their desperate searches for proper treatment and recognition. I feel extremely lucky: I sensed early on that whatever I had was too mild to be taken seriously, and so I simply got on with my life the best I could (and was lucky to be able to), finding my true friends along the way who could understand my inability to “come out and play” as an adult as much as everyone else. I also got a lot of counseling along the way that was validating, including some of the best I’ve ever experienced from Dr. Chino, one of the author’s of a great book I recommend: Validate Your Pain. It probably also helped that I asked for and attended a pain management class through my HMO over 7 years ago when I first suspected what I only knew as Hypermobility Syndrome at the time when I took out vertebrae T3-5 twisting while collating medical records of all things, not lifting, ironically. My great LMT at the time first helped me to suspect this after 3 different practitioners who were treating me at the time all independently called me very “plastic”, smile, and the description fit to a T, but my PCP wouldn’t let me see the geneticist yet. So I “sucked it up, buttercup” once again, got on with life, until my body demanded to be heard by falling copmletely and undeniably apart in early 2012 when you bet I needed some pain management! But as un-informed and short-sighted as my own doctor was for the last 15 years with me, my history with him helped him to know I certainly wasn’t lying when I promptly begged for an opiate to cope with my storm. (SI joint split on the right side, R leg subluxed, fingers, ribs and toes subluxed even in my sleep! Try a Blanket Booster if so.) I’m thrilled to report getting by with nothing stronger than Oxycodone for the most part leaving me with only occasional break-through pain, along with every flavor of non-opiate pain management possible: ice and heat, OTC meds (Tylenol and ibuprofen), a TENS unit, acupuncture, massage, Reiki, meditation, warm baths and water therapy, and my slow steady recovery via nutrition, especially increased Vitamin C, magnesium, calcium and zinc per my geneticist’s advice upon diagnosis. But I’m getting ahead of myself – I’ll share more on recovery techniques later. My point being, thankfully my long-doubting doctor knew me well enough to know and believe me when I did break down and beg for some pain medication, and also knew I wouldn’t abuse it (I never came close, and now take almost nothing unless I “bust a move” as I’m wont to do on occasion in my attempts to strengthen and have a bit of a life). Alas, not all are so”lucky” (or unlucky?) and are dismissed when they fall apart after many failed attempts to be believed.
But others have much more serious radiculopathies, neuropathies and neuralgias from their joints being misaligned and impinging nerves almost anywhere in the body, including the spine and sternum (yes, you can sublux your ribs in front, trust me! and yes it hurts!!) Sciatica and chondromalacia of all kinds is common, along with costochondritis and herniations of all kinds, and every flavor of spine trouble and resulting pain you can imagine. (Spinal stenosis, spondylolisthesis, sciatica, bone spurs, you name it!) We just don’t hold together! Just because a practitioner cannot see this on a scan or x-ray at any given point does not mean the pain isn’t very very real, alas. I now believe many drug-addicted street kids and homeless people may be self-medicating undiagnosed zebras since meeting a few this last year. This is why I’m trying so hard to raise awareness for all – I believe we could save our medical (and possibly judicial) systems millions in misguided testing and needless patient suffering and doctor-shopping if we just suspected this condition much more often than we do. That said, I am the first person to discourage drug abuse. But, I’m also leading the way in recovery from what I’ve observed also. (I now take fewer than 6 pain pills of any kind – even OTC – per month, if even that sometimes, depending on how often I try to bust a move with the newly rebuilt body).
Alas, this is apt to be an ongoing source of misunderstanding for too many for a long time to come, since pain doesn’t “glow”, so can only be reported subjectively. I assure you, no EDS patient I know wants to be on pain meds, nor seeks to get high. They just want their pain properly managed. (You don’t get high – and shouldn’t – if you are using opiates properly for pain management). Trust me, I’m thrilled to be able to manage with so little medication now. (I average a 3 on a 10 point pain scaleoverall, with a couple hot spots I might call a 6, and rare flare ups that drive me higher – and back to bed). I’m doing so on purpose, knowing full well things can flare at any time and I could suddenly need increased help, and so want to keep the “big guns” for only when I need them. But not all are so lucky, especially post-op in many cases. And they need to be heard. Not that it’s any excuse, but is it any wonder we lose patience with our mis-informed and sometimes short-sighted doctors when we’re suffering so? That said, we patients need to be as patient as possible while helping to bring our doctors and nurses with us on our diagnostic journeys as already stated in another post. It’s just very hard when you’re hitting a 9 on the pain scale. (I figure I’ll never self-report a 10, smile. I start bawling at 7 myself. Yes I’m a wimp, and proud of it).
Anxiety and Depression and Autism spectrum
 This last category is apt to be the most controversial, as most mental health patients and subclinical “auties” (autism spectrum patients – since we’re no longer allowed to call anything “Asperger’s” per the DSM V in 2014) are quite sensitive to the labels. Well, I’m sorry for your discomfort, but it’s emerging as an inescapable reality for virtually all EDS families in my observation on and offline in many support groups. My own perosnal experience and that of virtually every EDSer I know involves some level of depression, anxiety, codependency and any or all of the alphabet soup (OCD, ADHD, SPD, PDDNOS, etc.) that comes with being a subclinical high functioning autistic person, if not being outright clinical. (All zebras I know are related to or know someone on the spectrum, to my surprise, and the rest all battle the aforementioned alphabet soup until someone finally connects all those dots, if ever). Again, who knows why, but this is my personal observation of thousands of people and their behaviors and complaints online, including my own! (I battled severe depression through my 20’s). I now strongly suspect myself of being a “Hidden Aspie” in 20/20 hindsight since falling down THIS rabbit hole when a fellow zebra asked me about it 2 years ago. No, I’ll probably never get diagnosed – it’s much too costly and ineffective to attempt without a more “gross” presentation (again, so many are doomed to remain subclinical now, sigh). But all the tips and tricks for Aspies are working for me. Including strategies for coping with anxiety, stress, ADHD, etc.
This last category is apt to be the most controversial, as most mental health patients and subclinical “auties” (autism spectrum patients – since we’re no longer allowed to call anything “Asperger’s” per the DSM V in 2014) are quite sensitive to the labels. Well, I’m sorry for your discomfort, but it’s emerging as an inescapable reality for virtually all EDS families in my observation on and offline in many support groups. My own perosnal experience and that of virtually every EDSer I know involves some level of depression, anxiety, codependency and any or all of the alphabet soup (OCD, ADHD, SPD, PDDNOS, etc.) that comes with being a subclinical high functioning autistic person, if not being outright clinical. (All zebras I know are related to or know someone on the spectrum, to my surprise, and the rest all battle the aforementioned alphabet soup until someone finally connects all those dots, if ever). Again, who knows why, but this is my personal observation of thousands of people and their behaviors and complaints online, including my own! (I battled severe depression through my 20’s). I now strongly suspect myself of being a “Hidden Aspie” in 20/20 hindsight since falling down THIS rabbit hole when a fellow zebra asked me about it 2 years ago. No, I’ll probably never get diagnosed – it’s much too costly and ineffective to attempt without a more “gross” presentation (again, so many are doomed to remain subclinical now, sigh). But all the tips and tricks for Aspies are working for me. Including strategies for coping with anxiety, stress, ADHD, etc.
Along with seriously pathological codependency and narcissism IMHO. (You can tell a narcissist, you just can’t tell them much!) No wonder my parents were alcoholics, self-medicating trying to cope with so much pain and stress as I suspect in hindsight. But you absolutely cannot tell a narcissist anything about themselves, they will absolutely not want to hear it. (Mine sure didn’t). They will also often deny your reality, despite overwhelming evidence to the contrary. But denial (“de Nile”) is not a river in Egypt as we say in recovery circles with which I’m plenty familiar. And you don’t have to take my word for it. I’ll just keep observing everyone’s very black and white thinking patterns online, including, again, many in the medical profession. I think this definitely adds to the difficulty in getting EDS diagnosed – some narcissistc patients will not even see a doctor, others are doctors and nurses themselves (there’s a pretty high rate of EDSers in the medical profession, I’m finding, no surprise) and can’t see the forest for the trees right in front of them, alas. Again, being dialectic will help tremendously here, as everyone starts to just allow for the possibility that this comorbidity exists. (Again, why, I don’t know, but I have some personal theories I’ll share later! Some may even benefit greatly from dialectical behavioral therapy accordingly.) Meanwhile, autistic or not, I strongly suggest anyone battling anxiety and/or depression who is hypermobile (bendy) and experiences much pain at all look into EDS. Every zebra I’ve met in real life (IRL) exhibits fast thought and fast speech, high IQ (sometimes very), incredible creative talents (we’re some of the very best visual artists and musicians of all kinds out there, seriously!) We’re all very hard-charging, driven, often codependent, Type “A” high achievers – until our bodies betray us. (Trust me, I was one too!) And, EDSer or not, if you have these traits, you’ll definitely benefit from addressing the resulting issues. Your family will thank you! Remember, we’re really not that rare. So you’re definitely not alone!
Summary
Again, these are all just my personal unprofessional theories on the matter. Please consult a knowledgeable doctor for your case, but bring them some of the latest info (see my About post) in case they aren’t up to date yet to help if you suspect yourself now. But the more I observe in the support groups online, the more my likely “Aspie” pattern-seeking brain manages to file away in yet more categories. I’m not evening covering all the ways in which I suspect people, just some of the more common. You’ll notice that in all cases, everyone has some signs of GI involvement, along with allergy or MCAD signs, hypermobility, mood disorders, fibromyalgia and most common of all: widespread, medically invisible pain of every kind. We’re also finding virtually every diagnosed EDS patient and suspect EDSer can exhibit flying bird hand sign to some degree. It seems that even the least flexible zebras (of which Dr. Bravo himself is one – he says not all are bendy even as children) can bend their fingers back at the palmar knuckle to varying degrees. I have to try hard not to laugh out loud as some people I share my suspicions with will flash me fantastically bendy bird hand signs while emphasizing that they are not hypermobile! But don’t take my word for it. Start looking around. We’re the ones with the early onset varicose and spider veins, stretch marks in both boys and girls even at young ages, even if never large or pregnant. Often myopic (but not always), with crowded teeth and fallen arches, hemorrhoids, hernias and tendonitis and bursitis of all kinds. We just gotta get our doctors to recognize that elephant in the room that everyone is touching, from the podiatrist to the neurosurgeon. May your journey be smooth and filled with understanding. The good news: though there’s technically no “cure” (being a genetic defect), there are some things we can do about it besides just sit and suffer! I’ll be sharing more on that later.
Peeling the Diagnostic Onion

Diagnosing Ehlers-Danlos Syndrome

I have to say that I was slightly surprised to find that you’d been met by so much opposition from diagnosed fibro patients when discussing your theory. I was handed down a fibromyalgia diagnosis in January of 2012, and I’ve since found that the link between EDS and fibro is fairly irrefutable. I myself have nearly every symptom of EDS, from the major to the mundane, and I’m headed soon to one of the few true specialists in the country for an official diagnosis of type. I’ve even had symptoms eerily similar to the couple of your own that you’ve mentioned, including minor injury from over-rotation of (you guessed it) the L3, L4, and L5 vertebrae. (I also twisted my S1.) So far I’ve been officially diagnosed with Fibromyalgia, Raynaud’s Syndrome, Dysautonomia, IBS, Psoriasis, Migraines, Gluten Sensitivity, and Thyroid Disease (involving multinodular goiter), which ended in total thyroidectomy. I wholeheartedly agree with your theory and believe that all of these issues are associated with EDS. Please keep talking, even if it seems like nobody is listening. 🙂
Thanks Lulu – I’m glad you agree about my Fibro theory. But yes, strangely, you’re the exception. I think it’s because people have fought so long and so hard just to get even a fibromyalgia diagnosis, and it seems to fit “everything” they have (mildlly yet) so well, that they are understandably loathe to give it up. The other sticking point I see in person (because I’m dragging a leg and using a crutch) is they think: “oh, I’m not as bad as you, I am not visibly afflicted, so I cant’ have EDS”, which is so unfortunately mistaken. And b) they just simply have no idea what EDS is, and are so understandably burned out on people saying “have you thought about/tried X?” which have all turned out to be wrong. I know, I went through that experience myself years ago, so I just plain stopped talking about my complaints because I didn’t want yet another bit of unsolicited and misguided advice. I knew something was well and truly and deeply “wrong” with me (physically), but just didn’t know what. I’m strangely “lucky” that I became “visibly” afflicted and thus “clinical” enough to be recognized and diagnosed. I’m just trying desperately to get folks (doctors and our fellow reluctant and long-suffering patients) alike to connect the subclinical dots as you have. Glad you found me. Thanks for the encouragement! I will keep beating the fibro drum slowly but steadily with help from folks like you.
Hi,
I am hypermobile, have life long low blood pressure and many other symptoms of EDS (including blood pooling in legs and feet after showers, easy bruising, syncope and dizziness, chronic anxiety, IBS, sleep disorders and have just been diagnosed with Mast Cell Activation. Oddly though, I have very little pain (apart from horrendous headaches and get pain if I eat any of my trigger foods). Do you think this rules out EDS or do you think I may just be very lucky and not have much pain? Is there a test for EDS? I would like to get it done so that I know if my daughter is likely to have similar issues as my mother and grandmother all had these issues, although neither was ever diagnosed.
I still strongly suspect you despite your lucky relative lack of pain Holly – I’m finding all variations on a theme of sensory processing disorder to be commonly comorbid with this. And while some of us (myself included) experience lots of pain, maybe even more than average, some of us experience little to none. My friend Nova is one of these – she discovered this after she started taking L-Arginine and suddenly felt ALL KINDS OF PAIN! So she stopped of course, cuz… ouch! We may all just be wired differently, and this is part of what makes it SO confusing for doctors: to some it just looks like party tricks, but for others, it’s a disabling painful condition. The rest smacks of comorbid MCAD of some kind generating some dysautonomia.
Anyway, I highly recommend this post for how to pursue a diagnosis, bearing in mind the criteria may change soon (in March 2017 we think) when the working group publishes their latest consensus. Until then: http://ohtwist.com/about-eds/diagnosing-eds/
There is no single easy “test” for EDS. You have to suspect what type you might have, while also ruling out any other heritable diseases of connective tissue like Marfan Syndrome or Stickler or OI which have a lot of overlapping symptoms with us. Then, if you still suspect it to be a form of EDS, if it doesn’t easily match one of the more rare forms you can only be diagnosed clinically (subjectively) using the Brighton Diagnostic Criteria (for now). So sorry, not an easy diagnosis. I highly recommend trying to see a savvy medical geneticist for this reason after gathering as much family medical history (everything, even things you think are not related) as you can to help them diagnose you. HTH. Good luck. (It’s not rare, it’s rarely diagnosed.)
Recently managed to finally get a fibro diagnosis here, and I def meet the criteria on the Brighton’s thing too, even with no clue what my Beighton’s score is. In case you wanted another datapoint XD
Personally I’m not actively resistant to considering EDS, but… when the type I would most likely have also has no definitive test, I just really get the strong feeling that it would be a very bad idea to start up another such campaign so hot on the heels of my last one, y’know? Like, I was so sure it as fibro, it feels like turning around now to say “Oh but EDS” would get even my blessedly more sensible current GP stamping my file with “hypochrondiac”.
I’d totally buy fibro as an early form of EDS, though. For all that I definitely had a storm of my own (I’m stealing that term now btw, it’s such a perfect word to describe the feeling of that crashing conglomeration of ill health), it did largely seem like a sudden escalation of lifelong problems, not new ones, and my biggest hesitation around EDS is that I don’t feel like I’m “bad enough” to count.
I understand that sort of “imposter” syndrome – I had it too at first, even after I landed in my wheelchair (stopped being able to walk at all) in early 2012. Like, just what else could it be? I knew it wasn’t MS etc. Nor an illness (I didn’t have swollen glands and a fever.) I had also suspected the condition for the prior five years since injuring my thoracic spine twisting, collating medical records, not lifting, ironically.
And I thoroughly understand not wanting to be labeled a hypochondriac – a much too common experience for us. Especially after just fighting to get the fibro diagnosis. But do know that not all who have hEDS have many problems, ironically. It’s a weird diagnostic schema they’ve hatched: trying to claim hEDS isn’t worse than the new HSD category (which you may better fit, btw) but can be equal in severity etc. However, it’s so clear that HSD is perceived as “less than” since you just plain don’t tick off as many boxes on the list. All normal humans would naturally assume that’s less serious or severe. It’s human nature. I.e, you don’t have to be “that bad” to count, no, but it’s easier to get diagnosed if you are. (As happened to me.)
That said, I think you could maybe just wait a year or two, and slowly drop hints to your new sensible GP until you feel like enough time has passed to logically say “Hey, what do you think of this proposition?” and drop them the EDS Toolkit here: http://rcgp.org.uk/eds to check out when you finally do bring it up. The treatment is ultimately the same in the end: triaging injuries, good nutrition, sorting your sleep and pain management, and staying as active as you can stand to. (Heh. Not easy, trust me, but we gotta do it to have any quality of life.) Anwyay, glad you stumbled on my site. And, you are now tapped into all the latest info whenever you decide to pursue it. You could maybe start gathering family history in the meantime as I suggest here in “How to Diagnose” to help you later. Cheers.
Thank you so much for this!
A few people have told me they suspect I have EDS. And I am looking for a doctor who can check if I actually do have it or not.
A lot of the things you mentioned in here, I also have. I am autistic, I have a depression and anxiety disorder, I have IBS, joint hypermobility, chronic pain (I have a fibromyalgia diagnosis), an auto-immune disease, trouble falling asleep and staying asleep. I hope I can find a doctor who will actually take me seriously, because the last Rheumatologist told me I’m ”just hypermobile” and didn’t even want to speak about HSD much less EDS. When I asked her about EDS she said I couldn’t have it because I have never luxated a joint. While my jaw, knees and fingers subluxate almost every single day.
So thank you again for this. I feel less like I’m just whining and trying to get attention.
You’re most welcome Suzan. And alas, your experience is all too common in our community I’m finding, autistic or not. (But especially if so – this seems to get us even more dismissed than others I’m finding.) Regardless – I strongly suspect you based on this short description, but as I’m not a doctor, and haven’t examined you properly I can’t be more definitive.
I have noticed a tendency for rheumatologists to strongly resist updating their knowledge base, and stick to either old outdated information as yours just did, or only recognize and diagnose highly co-occurring autoimmune diseases. Which is really unfortunate, since they see us the most! (We ARE the frequent flyers in rheumatology offices!) I would try to see another doctor if you can manage it – most are working off of quite outdated information. Try to find a local support group to help with finding one who will or is more up to date. This site might help with that:
https://chronicpainpartners.com
And, here’s another good post to help you further suspect yourself and your family, and gird your loins for the next doctor:
https://ohtwist.com/when-else-to-suspect-ehlers-danlos-syndrome
And my recommendations for how to go about getting diagnosed:
https://ohtwist.com/about-eds/diagnosing-eds
For what it’s worth, I find all of the following highly co-occurring in at least our biological families, if not even all in the same patient sometimes, yes, quite a burdensome package:
https://ohtwist.com/the-chronic-constellation
Just know you are NOT alone, I (and many others) feel and believe you. And to stay strong and have faith – with persistence you will eventually get properly recognized and diagnosed. Stay strong! You are not whining!
Well just found your website by putting some crazy unrelated keywords like
“ADHD Ehler Danlos Intelligence” after having 3 days of not sleeping and started feeling pain on my body.
LOL I am not diagnosed by EDS (yet) bc I never checked before, I was scared to know if I have it, right know with you agreeing I have less hopes. But I am surely gonna take better care of myself. So, It was fun to read your post… And noticed in comments I am very similar to you all. Except in general I don’t have pain, (probably bc i have high tolerance to pain; I love spicy food the most)
Iam 22 years old; I have 2 slipped disks on my back :’D never broke a bone (except the time I literally smashed my finger like a bombed sausage)
Literally my feet once got stucked to bicycle wheel when I was a kid and it got curved like a “Cavatappi” but not broken.. haha… and I don’t know what to do now, I am quite lost rn… I was freaking my freendz out by doing weird things with my body… And I was a proud weirdo… I still am… Maybe that pain won’t go worse ;;;;;D
I so feel like a spider in the middle of a world wide web of words sometimes, slowly catching my unsuspecting “prey” (potential fellow EDS/HSD/MCAS etc. sufferers) one by one through all these searches! Welcome to my “web”, and yes, I’m sorry to say that not experiencing much pain does NOT mean you’re “safe” from a Hypermobility Spectrum Disorder (invented in 2017) or EDS alas. For some odd reason, some folks don’t experience much or any pain. I don’t want to alarm you, but all the ones I know are either diagnosed with or strongly suspecting the rare form called Classic-like EDS (not Classic or Classical EDS aka cEDS), aka. clEDS. It seems they may lack full enervation of their bodies, lending to both that low pain sensation (silver lining), but also other issues, such as familial dysautonomia (not the same as POTS) that’s highly co-occurring in these families especially after any major viral illnesses. (We don’t know why.) But, this is NOT a diagnosis to be clear, just an explanation of low/no pain in some EDS patients I know of.
I highly recommend this page for pursuing your suspicions further with the aim of getting diagnosed if that’s what you do want eventually:
https://ohtwist.com/about-eds/diagnosing-eds
And this page to continue helping to suspect some kind of connective tissue disorder, whether a form of EDS, or HSD, or another, similar Heritable Connective Tissue Disorder like Marfans, Sticklers or Loeys-Dietz e.g. (Do thorough work up to rule those out if you can. Many get misdiagnosed with EDS to start.)
https://ohtwist.com/when-else-to-suspect-ehlers-danlos-syndrome
You’re in good company! I’m just now realizing ADHD is highly co-occurring after all these years. (I was distracted by autism at first, in 2012, but now see ADHD just as common, frankly, with many of us having a combo even, some call “AuDHD” now. I’m sure there’s lots of overlap, with just a handful of folks at both extremes. But that’s just guess to be clear.)
Omg this…it’s as if I’m reading a page from my own book. I have so so so many of these symptoms: migraines, ADD, muscle/joint pain/stiffness, severe chronic pain, varicose veins, stretch marks (started at 12 yo and continue), osteoarthritis (in my 30s!), TMJ, sleep issues and stretchy skin. I’m not sure about loose joints but I did get a massage today and when I got up…every joint in my body popped loudly…I have other health issues related as well i just cannot list them all! I was called a hypochondriac my whole life by my mother so I guess that’s why I don’t complain, but I am miserable!
Then I probably shouldn’t share my “When Else to Suspect EDS” page with you, or you’ll be sunk, smile! 😉
https://ohtwist.com/when-else-to-suspect-ehlers-danlos-syndrome
Welcome to “Clan Dumpty”, of Humpty, fame, right? We’re a huge global “family”. And no one can put us back together again, or not easily.
“If you can’t connect the issues, think connective tissues” – anonymous, as quoted by Dr. Heidi Collins in her talk with that title in 2014 at the EDNF Conference. (No longer on YouTube, alas, it was really good.)
Anyway, to quote MCAS specialist Dr. Afrin, “do you really think there are 57 different things wrong with your patient, or might there be just one or two underlying systemic issues driving it all?”. Nope, you’re not losing your mind, just your body… 😉 Welcome.
Mast cells do not line the axons nerves, as far as I’m aware. They are surrounded by nodes of insulating fatty cells that help the nerve impulse skip along faster.
I found this very illuminating. It’s nice to see someone else drawing these connections. Maybe I will try to get diagnosed. It’s fucking hilarious that you accuse doctors of having black-and-white thinking and unacknowledged autism. I don’t disagree.
I appreciate your insights on mental health. This is such a great website. Thank you.
Yes, all nerves (axons) are coated in myelin sheaths. (Or should be! You’ll have problems if they’re not.) But… those sometimes sport mast cells. There is an interplay, for our lose, unfortunately. Glad you like the site. And yes, some doctors are probably also autistic and or have rigid black and white thinking. I know, I’ve suffered at the hands of many personally. Cheers.