Potential biomarker for hEDS and HSD found
News broken September 11, 2024: Potential biomarker found that may allow for easier diagnosis of hEDS and HSD per The Ehlers-Danlos Society. (Me Jan: hold your zebras folks – this result still needs to be CONFIRMED, and then reproduced and then made commercially available, but it portends the possibility sooner than later, yes! Exciting!)

I don’t have to tell most of you how momentous this news is. Not only does it portend a much easier diagnostic process and less medical gaslighting for all of us some day, but it also confirms what I’ve suspected all along: that HSD and hEDS are probably just subsets of the same thing. And then perhaps we can recombine them and thus REDUCE THE COMPLEXITY to the current diagnostic process I just wrote about recently on social media.
I just added a diagnostic flow chart to my Diagnosing EDS and HSD page to be clear, so as to make it easier for doctors and everyone else to not miss any steps in the process. There are a LOT of steps and conditions to wade through presently, after all. As shown in this screencap of that table here:
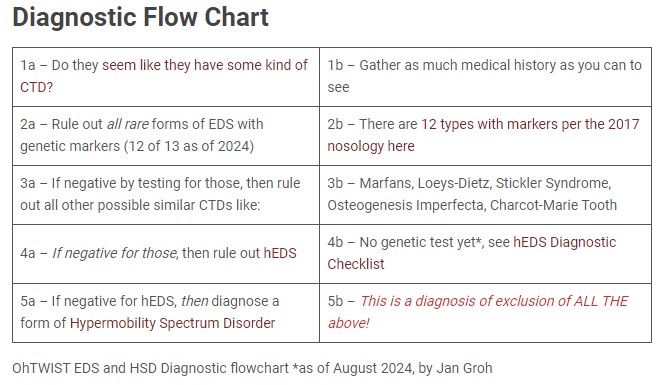
Image ID: Diagnostic Flow Chart above a table with rows reading:
- 1a – Do they seem like they have some kind of CTD? 1b- Gather as much medical history as you can to see
- 2a – Rule out all rare forms of EDS with genetic markers (12 of 13 as of 2024) 2b – There are 12 types with markers per the 2017 nosology here
- 3a – If negative by testing for those, then rule out all other possible similar CTDs like: 3b – Marfans, Loeys-Dietz, Stickler Syndrome, Osteogenesis Imperfecta, Charcot-Marie Tooth
- 4a – If negative for those, then rule out hEDS 4b – No genetic test yet*, see hEDS Diagnostic Checklist
- 5a – If negative for hEDS, then diagnose a form of Hypermobility Spectrum Disorder 5b – This is a diagnosis of exclusion of ALL THE above!
* – as of August 2024 by Jan Groh.
Obviously, this could all become deliciously obsolete some day! BUT, and this is a big but, not so fast, PV.
Here’s the thing, not only do they need to still confirm this research finding (though you bet we’re gonna be all over them to do so like bees on honey), but… I wish to humbly propose yet another consideration:
It is not impossible for someone to have BOTH a form of hEDS/HSD AND a more rare genetic form of EDS and or other CTD. So, someone could test positive for this biomarker, but again, if the doctor stops short after that finding, they may miss other co-occurring forms of EDS or other CTDs as shown above.
Why do I say this? Because… it’s been proven in the past that people CAN HAVE MORE THAN ONE TYPE OF CTD in the same person. I met someone at the 2013 Oregon Conference I personally organized and held in Portland with Dr Byers and more. He asked if anyone had more than one type confirmed by genetic testing and about three people answered in the affirmative. One next to me had both Marfan Syndrome AND classical or vascular EDS if memory serves. Yes, confirmed by a geneticist. Is it rare? Sure. But not unheard of.
If you simply test for this new biomarker and then stop? You may still miss these other co-occurring conditions! So, in my opinion, I think we should STILL do proper differential diagnosis for all the forms as shown above, then run the new biomarker test to rule out hEDS/HSD as well.
Yes, even if you diagnosed a rare form by genetic testing like kEDS or vEDS. Toss in the hEDS biomarker on top, to make sure that’s not also a factor for them! (I really do believe it’s possible to have more than one type, but probably not more than two to be clear. Not sure we would be biological viable with more.)
And, we still don’t know what lies behind hEDS/HSD, even if we may have found a biomarker. (Which is a result of it.) Is it one main gene or gene family such as that Kallikrein gene found by the Norris Lab at MUSC? Or is it a combination? Or what?
We truly don’t know yet.
I’m quite sure we’ll keep peeling off various small subsets of folks with unique rare genes like the MIA3 found in Poland in 2023, and the Kallikrein gene found by the Norris Lab announced earlier this year (June 2024). But neither of these (or even the combo) fully explains the whole pool of hEDS/HSD patients in my opinion. Still.
We don’t yet know what else is involved or driving. But I’m cautiously optimistic and excited that more candidates are going to be found in time. I will write more about this on my Patreon page soon.
Meanwhile, I’ve felt strongly since the Hypermobility Spectrum Disorders were “invented” in 2016 by a committee of self-appointed experts and not backed by any medical science, that they might not be really different than hEDS. Just subsets of presentation of hEDS.
I feel like we keep getting hung up on classifying and categorizing things so much that we keep missing the forest for the trees. Much like has happened with autism all these years: the original criteria were based on a subset of mostly white boys, and all other phenotypes in all other genders missed until lately.
I feel like we’re doing the same with hEDS, only in reverse: describing primarily thin, Marfanoid-like cishet white females, to the exclusion of all other body types and presentations. I truly think it runs in men and boys and other bodies just as much – but just… differently. And like autism, it should not be gendered either. I have trans-men friends who have admitted that their bodies tightened up a bunch after they started Testosterone (T) after all. But they were diagnosed with hEDS before transitioning. They might not pass the test after.
So, think outside of your rigid diagnostic boxes please. Open your minds and eyes to other possibilities. Come up the mountain, above the timberline and see the forest for the trees with me. The view is fine.
Changes coming to EDS classification December 2026

Gaslighing Syndrome
