What is MCAD (or Mast Cell Diseases)
“I have or suspect I have Fibromyalgia or a form of Hypermobility or Ehlers-Danlos Syndrome or lipedema or Dercum’s. So what is ‘MCAD’ and why should I care?”
Well I’m so glad you asked! In short, it’s because we’re finding a vast majority of patients with some form of hypermobility, whether full-on Ehlers-Danlos Syndrome or the new category of Hypermobility Spectrum Disorders (announced March 2017) also have signs of comorbid MCAD. (The “A” is for “activation”.)
EDIT September 17, 2022: I interrupt this introduction to bring the new insight that the term “Mast Cell Diseases” or MCD appears to now be the proper over-arching umbrella term for all the forms of Mastocytosis as well as all the forms of MCADs – which includes MCAS, HaTS and MMAS. My apologies for lending to anyone’s confusion. I will be slowly editing and updating my site to reflect this as per this recent 2022 article.
Including the quite rare mast cell leukemia, all forms of Mastocytosis (several, including systemic and cutaneous forms) and the newer least known but most common Mast Cell Activation Syndrome aka MCAS of some kind, and vice versa. I personally include all patients with Fibromyalgia, as I again find a majority of them show signs of a hypermobility spectrum disorder or hEDS.
So much so, that Dr. Josh Milner at the NIH actually studied this comorbidity (of atopy (allergic disease)/MCAD and HDCTs like EDS and the resulting dysautonomia including POTS) for any genetic connection, concluding in 2016. (They got my blood in latter 2012 toward this end among others.)
And for those of you who don’t know about the Ehlers-Danlos Syndromes or Hypermobility Spectrum Disorders yet, I hate to share that we’re finding them to be very commonly co-occurring with all forms of MCDs, even if not 1:1.
Dr. Milner’s study did find a subset of patients who exhibited an elevated baseline tryptase in a familial inheritance pattern, who all also exhibited signs of hypermobility characteristic of hypermobile type Ehlers-Danlos aka hEDS and many of the comorbidities. This has come to be called “HaTS” in the mast cell community, or: Hereditary Alpha Tryptasemia.
That said, not all patients with hEDS have an elevated baseline tryptase, and I don’t believe all patients with an elevated trpytase are also hypermobile – he only studied those who are. You can learn more about this subset here:
- NIH Scientists uncovering genetic explanation for frustrating syndrome Oct 2016
- One Gene Mutation Links Three Mysterious, Debilitating Diseases 2016 (Mental Floss)
- FAQ’s about the above from the NIH 2020
Many other patients (including me) still have what we affectionately call “The Trifecta” of EDS, MCAD and POTS or other dysautonomia forms still, even in the absence of “Familial Tryptasemia” or HaTS. Again, it just explains one small subset. We still need to explain the majority, and more.
Update 2021: There is now a commercial test available to see if you have HATS here from Gene by Gene. Talk to your doctor to get it ordered.
Allergies and Sensitivities
Patients with MCAD are those people who may have some (or even lots of) “traditional” common IgE-mediated pollen, food and drug allergies, though not always! Many are totally negative for any “traditional” IgE-mediated allergies you can test for.
But we often also have additional food and drug and environmental sensitivities and intolerances (IgG and IgA mediated reactions that don’t tend to require epi-pen use) AND…
…many reactions of any severity (including any grade of anaphylaxis) to foods and drugs and also non-proteins like scents, dyes, chemicals, sunlight, vibration and stress not explained by either IgE or IgG as well. This even includes electromagnetic radiation for some.
{kind=link}
Some get mis-diagnosed with “multiple chemical sensitivity”, porphyria or idiopathic anaphylaxis among other things besides the common throw-away mental health diagnoses of depression, anxiety and hypochondria. Those in a hurry to find the best articles for your doctors, please see my MCAD Resources, else read on to learn more about MCAD and when to suspect it.

We are often allergic to bee or wasp (hymenoptera) stings and anesthetics and contrast dyes (notably iodine), sometimes vomiting for days after some procedures. We may also have idiopathic (meaning: unknown origin) hives, mad itching (anywhere, can migrate), rashes, flushing, sweating, sudden onset diarrhea, gas, bloating, cramping, asthma, wheezing, blood pressure drops and/or spikes, esophageal spasms, headaches and much more from MCAD.
Toss in commonly comorbid POTS, and we call it winning the “Trifecta”, smile. This combo (EDS/MCAD/POTS) is proving much less rare than first thought, too, alas. Some patients are lucky to be upright and breathing normally at all!
You know that “food coma” you get after your large holiday dinner? For most it’s just the effects of eating a larger meal than usual on most humans as a lot of blood goes to your gut to aid your digestion. (They’ve proven that the tryptophan in turkey is negligible and not likely the actual cause of any sedation.)
But in MCAD patients, you may actually pass out after eating any number of triggers and even in small amounts, literally, albeit looking like you’ve fallen asleep. (We affectionately call these “masto comas” in the groups, but that is not an official medical term, so don’t use it with your doctors!)
This is because we get to enjoy more sedating effects from added mast cell activation that leaves you feeling “rhino darted”, like you’ve been literally tranquilized sometimes. (Often if you wait too long to eat, and then eat a lot all at once. Low blood sugar can trigger us also, and often before it’s measurably low in the clinic.)
The experience or effect seems identical in my experience to opioid-induced respiratory depression, but happens even in the absence of opioids, and to many other triggers I find. (Sunlight does this to me, no kidding, along with vibration on road trips.) I find my breath rate goes down to just 2 or 3 per minute sometimes. But I always thankfully come back after about four to six hours.
I’m currently at a loss to explain how or why this respiratory depression (hypoventilation) happens in the absence of opioids, though theories have ranged from prostaglandins released by our mast cells as shown here and here to excess histamine crossing the blood brain barrier (no citations found yet). I find this last idea confusing since I thought histamine was arousing, but what do I know? (Further enlightenment and theories from smarter folks quite welcome!)
I’ve found nothing that works to counteract it for myself yet though one friend benefits from Benadryl lending credence to the latter theory, but this article leads me to wonder about Naltrexone (regular or low-dose) as a possibility now… but I digress.
Many react to alcohol also, which may lead to our wonderful reputation as “alcoholics” who can’t hold our liquor. (Just one drink gives me a bright red nose and puts me out now! Needless to say I don’t drink anymore. Most with Rosacea show signs of MCAS.)
I didn’t even realize I had actual food sensitivities until I saw a naturopath in 2012 to address my increasing Irritable Bowel Syndrome (IBS) post EDS onset “storm” of February 2012. I now feel strongly most IBS is a combo of food and drug allergies, SIBO, candidiasis, leaky gut and sensitivities or some form of MCAD. This makes sense in light of our weak ileo-cecal valves, soft inner tissues, weak epithelial layers, weakened immune systems and who knows what else.
But again I digress. Here is a handy pdf of the more common MCAD Symptoms List with some useful links I ran past The Mastocytosis Society in 2012. I really like the Canadian Mastocytosis Society’s web page on same as well. I also think MCAD and Histamine Intolerance may well drive some emotional & mental health disorders also via histadelia from excess histamine, but that’s just my humble opine.
And this can and does highly resemble Histamine Intolerance, which is technically a condition where you don’t necessarily produce too much histamine from over-active mast cells as in MCAD, but you lack the enzymes (DAO, HNMT) to out-process it sufficiently to keep up with normal levels of production. And… a la Hickam’s Dictum, yes, some if not even many patients may actually have both. The Low histamine Chef can tell you all about her experience finding this out the hard way.
A low histamine diet can be helpful in all cases, but may not be sufficient or helpful for those with true MCAS or Mastocytosis for whom specific trigger avoidance is key whenever possible and additional mast cell stabilizers may be necessary among other things.
Further, it may needlessly restrict your nutritional intake I.e, you may still be badly triggered by a technically low-histamine food, which makes it a moot point since for you, it still produces histamine from your added reactivity. This is also why I do not list specific foods to avoid or diets to follow aside from some categories – it’s as individual as fingerprints, just like EDS is.
America’s Pharmacist Suzy Cohen RPh also explains some other ways to tell the difference between true allergies and excess histamine (though she notably omits any mention of any form of MCAD) here.
Now for some basic terminology and science behind MCAD.
What are Mast Cells
Mast cells are a form of “sentinel” cell in our immune system, and serve a very useful purpose in warding off bacteria and infections especially at sites of wounds or entry.

They are born in our bone marrow, but are kicked out relatively “young” in their lives while immature and undifferentiated, and migrate through our blood and into our tissues, ultimately lining all of our external facing tissues including our skin, eyes, lungs, ears, nose and GI tract from lips to tail. (Food is an external substances rife with bacteria after all, so our GI tract is still technically externally facing.)
But they also have been found in the linings of our brains and our hypothalamus, where they seem to wreak havoc with our endocrine systems and cause lots of brain fog and related effects (seizure activity, speech loss). They are also known to line our blood vessels, causing vaso-dilation (opening of the vessel walls allowing plasma leakage called third-spacing) or angio-edema when activated around them.
They are small blob shaped cells filled with small “granules” that contain or produce over 100 various chemicals and proteins celled “mediators” that are released upon being triggered by an infection or wound or antigen or other trigger. This produces what we commonly term “allergies” or allergic like reactions and symptoms and chronic inflammation even in the absence of IgE antibodies the allergist can test for.
The most common of these mediators include histamine, leukotrienes, prostaglandins, tryptase and cytokines. (Cytokines are really a class of very short-range fast acting chemical messengers between cells, kind of like blue-tooth is for your computer.) This is why anti-histamines help with our allergies – allergens trigger our mast cells, releasing lots of histamine which make us sick and tired as too many well know. Anti-histamines serve to block the histamine receptors on all of our cells, reducing this effect to more manageable levels.

This also is why we turn red at the site of a cat scratch or mosquito bite or cut. Mast cells can also recruit more mast cells to such sites as well as eosinophils, another type of granulocyte akin and attracted to mast cells. Eosinophilic esophagitis among other EO disorders are also fairly common among us, no surprise.
Mast Cells also may not always fully degranulate from a trigger, but rather “leak” a few mediators at a time, and possibly even when untriggered in some of us. Full degranulation usually leads to life-threatening “Stage IV” (highest grade) anaphylaxis. Some patients refer to themselves as “leakers” vs “shockers”. I’m a lucky “leaker”so far, knock wood. I tend to avoid full epi-pen warranting anaphylaxis as long as I keep my overall histamine & stress levels down, and avoid iodine contrast dye.
What is MCAD
Technically, “MCAD” or Mast Cell Activation Diseases is the umbrella term for the collection of mast cell diseases that range from the thankfully extremely rare Mast Cell Leukemia (an actual rare blood cancer requiring chemotherapy like Gleevec to control) to the less rare but still uncommon forms of Mastocytosis in the middle, to the newly recognized but very poorly known but (like hEDS) much less rare, and much more common MCAS or Mast Cell Activation Syndrome, for those who test “negative” for actual Mastocytosis but, as leading MCAD specialist and hematologist Dr. Larry Afrin puts it so well: “walk like a duck and quack like a duck”. To which I like to add: “and suffer like a duck” TYVM!
In other words, you may have many signs and symptoms of a form of Mastocytosis, but be negative for it based on serum mediator levels or biopsies for mast cells. But you are still going anaphylactic to varying degrees or reacting to a myriad of triggers, from foods to scents to stress to hormones. Thankfully the TMS helped produce the ICD-10 codes for diagnosing it that were released finally in October 2016. (Now doctors have a billing hook to hang you on so to speak.)
Dr. Mariana Castells of the Brigham and Women’s Hospital Center for Excellence for MCAD explains this quite well in this video from March 2014 via the CSF. It can also exacerbate any underlying POTS or other dysautonomia quite nicely too, unfortunately. (Adds to BP drops, weakness, fatigue.) You might also want to check out my Intro to MCAD talk given June 2015 or the recent NEJM article from 2015. (Yes, you need to subscribe to that for access. Ask your doctor or a medical library for help with this.)
Mastocytosis
With the various forms of Mastocytosis, your body produces too many mast cells (a neoplastic or myeloproliferative condition) which may also be over-reactive (trigger-happy) which then migrate to various places including the skin and GI tract and set up camp in distinct clusters that can sometimes be visible to the naked eye on the skin in the form of urticaria pigmentosa – basically hive like brownish red patches or spots that persist (unlike hives which come and go completely with no trace left), though they may fade between flares and triggers. (MCAD patients should not donate organs or blood for this reason – you don’t want to share your “bad” mast cells with a recipient!)
But not all will have cutaneous aka skin signs. Some will be seriously affected in the GI tract requiring upper and lower endoscopy to find (if you’re lucky and they happen to hit the right spots in your body – not all succeed). This is indicated in patients who are suffering terribly from seemingly “idiopathic” (cause uknown) GI pain, malabsorption, IBS, nausea, constipation and/or diarrhea that can be quite show stopping and disabling, never mind socially isolating.

Some react to all but a very few foods despite testing negative for actual food allergies. They can and will experience a lot of anaphylactic episodes, not all of which will be throat-closing and often involving psychiatric involvement and thus not always recognized for what they are. Anaphylaxis actually comes in grades based on the number of body systems involved and to what degree.
Most EMTs and doctors only recognize the highest/worst level or throat swelling as true “anaphylaxis” at this time and dismiss many other signs and forms. My fellow patients have learned to just talk about their symptoms and be mentally prepared to “tip over” to full-blown ana based on their body’s history of same, no matter what anyone calls it. (Keep those Epipens handy!)
The diagnosis includes testing serum tryptase levels both at “baseline” or on a “good day” (if you can find one!) and during a flare or when triggered for comparison. Triggers can be environmental as well, not always just foods or drinks among other mediators.
Yes, this can be extremely tricky to manage for both patient and doctor, as one can’t always predict when a flare will occur and not all elevate much if at all even then. (Many can’t get off the toilet long enough to get to the lab to test at such times.) And some will undergo a bone marrow biopsy (BMB) to try to find “patches” of mast cells there when suspected also. However, a negative BMB does not preclude having Systemic Mastocytosis. It can take up to six BMBs to hit the right “patch” even in those who do end up having Systemic Mastocytosis, so even this test is not 100% reliable as described here. You may end up just waiting and watching to see if your disease feels like it’s progressing. (Not all do, nor do all progress to mastocytosis, or maybe not in a measurable way at least.)
Mast Cell Activation Syndrome (MCAS)
As mentioned MCAS on the other hand is what is diagnosed in patients who suffer much like Masto patients do from “trigger-happy” or over-reactive mast cells, but show no signs of increased numbers or clusters of them anywhere, making it even harder to diagnose. Your biopsies if any will be negative for notable clusters or deformed cells, and serum tryptase and other mediator levels may still be low even during reactions. But, you can and may be just as anaphylactic (or anphylactoid) as a Masto patient just the same thanks to your over-achieving mast cells. (I keep trying to put mine in a time out, but no dice yet, sigh.)
We are those people who tend to have lots of signs of food allergies, and systemic inflammation (itching, eczema, hives), headaches from increased hydrocephalus or IH (I call mine “brain juice headaches”), flush red easily especially from the neck up especially the ears, have exercise intolerance, have BP drops or spikes, nausea, constipation, or sudden onset diarrhea after ingesting certain triggers. I get painful esophageal spasms (diffuse and “nutcracker esophagus) if I eat some triggers, or when stressed or eat too quickly.
We can also be triggered by stress, heat, cold, lights, smells and startling sounds. I found myself going anaphylactic in my power chair in the winter of 2012 while waiting for the bus – who knew! I also started degranulating from the vibration the last time I rode in a turbo-prop plane during a short hopper flight back east at a conference. I have my online support groups to thank for helping me figure that out and saving Kaiser thousands of dollars of needless testing. Flares often worsen during a woman’s menstrual cycle also. Progesterone makes you more lax and I just learned is also a MC trigger (2016), and estrogen seems to increase the mast cell activity also.
But men and boys suffer plenty too, alas. And of course some people who land in the middle will also “enjoy” some of these issues and symptoms depending on their phenotype (biology). Some trans and genderqueer persons have both sets of sex organs to varying degrees. Or can appear male, but cycle like a female, or experience the same hormone surges despite appearances. Never assume.
MCAS is one of the hardest conditions to diagnose at present however, as there is no single “pathognomonic” or tell-tale test for the condition. Further, you often may not show elevated levels of serum tryptase, the most common mediator tested for diagnosing Mastocytosis, which is what most doctors will first suspect or ever consider. Many doctors have not yet heard of MCAS so will only look for Mastocytosis yet.
But, you will often (but not always) show elevated urine histamine or Prostaglandin D2 metabolite levels over a 24-hour period among other things. Though it is key to keep these specimens well chilled at all times as some of the mediators disappear within 2 minutes at room temperatures, leading to loads of false negatives.
Much like how Mastocytosis used to be only diagnosed at autopsy 30 years ago until some medical examiners got smart and asked where the patients were before they died and they found clusters of mast cells and mastocytomas in them, MCAS is even less well recognized, since it generally is not quite as obvious with no tell-tale spots to biopsy, though it can still be plenty disabling and show stopping, trust me. We have also “normalized” it in society – this is what many drug companies are targeting in ads for TUMS and Nexium. It’s just that now we may have a name for what’s driving all that GERD and heartburn!
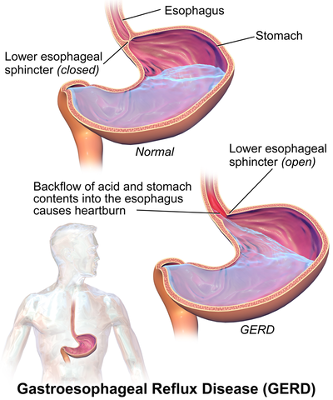 Some doctors are (wisely IMHO) starting to diagnose MCAS presumptively (or clinically) based on symptomatology (patient complaints that match) and response to the standard therapy for both conditions presently: trigger avoidance, and use of mast cell stabilizers and H1 and H2 blockers, aka anti-histamines. H1 blockers are your standard OTC allergy products like Benadryl, Zyrtec, Claritin, etc., and H2 blockers are for the stomach receptors, such as Zantac or Tagamet, as the stomach produces acid in response to histamine levels – combine that with weak hiatal sphincters or the ring-shaped muscular “valve” between esophagus and stomach in EDS patients and there’s an explanation for much of our “GERD” in the EDS community, IMHO. I’ll say this much, mine has vanished since eliminating some key triggers for the win. (Coffee was a big one for me.)
Some doctors are (wisely IMHO) starting to diagnose MCAS presumptively (or clinically) based on symptomatology (patient complaints that match) and response to the standard therapy for both conditions presently: trigger avoidance, and use of mast cell stabilizers and H1 and H2 blockers, aka anti-histamines. H1 blockers are your standard OTC allergy products like Benadryl, Zyrtec, Claritin, etc., and H2 blockers are for the stomach receptors, such as Zantac or Tagamet, as the stomach produces acid in response to histamine levels – combine that with weak hiatal sphincters or the ring-shaped muscular “valve” between esophagus and stomach in EDS patients and there’s an explanation for much of our “GERD” in the EDS community, IMHO. I’ll say this much, mine has vanished since eliminating some key triggers for the win. (Coffee was a big one for me.)
My doctor and I found this document to be the most useful for my MCAS diagnosis. I also just discovered this great blog post on diagnosing MCAD of all types that shows just how challenging it can be. (You can still have Systemic Mastocytosis even with a negative bone marrow biopsy!) There are several other helpful documents on my MCAD Resources page.
I’m going to stop there for now, and provide additional information in some subpages to help keep folks from being overwhelmed. (Possibly, too late.) Having the “Trifecta” is seriously like falling down a rabbit hole – with several other rabbit holes attached! I.e, it can feel never-ending, and in some ways it is.
But… it can really help to know you’re not alone in your experience (finally, ahhh!) and are not “just sensitive”. Or rather, you are, but now have a medical explanation for it! Toss in that mast cells line our nerves and can contribute to increased pain as well as neuro-inflammation, aka “brain fog”, and no wonder we suffer so badly from seemingly “minor” insults. Ah, if only pain glowed! My doctors would all be asking me my secrets for coping so well, I’m sure! (And dousing me with a water hose.) Try, we don’t have much choice! And you might want to join the Yahoo Group called The Elephant Project to continue pursuing all of this further with fellow patients who are seeking and sharing answers for same.
Thanks for all this info. I’m newly dxd hEDS w IIH, Dysautonomia and what I believe is a raging case of MCAS. My head is spinning…..not sure what to do. Blah.
You’re welcome. I’m sorry it is so, but better the devil you know eh? Ironically, my MCAS is my most debilitating condition now. Oh sure, my bones come apart easily, I can stil move them with my own hands (self-subluxing anyone?) but that pales in comparison to the pain and side effects of my MCAS flares OMG. Which while all Level I (no emission, or not many), are still quite show stopping. Anyway, know that there’s a lot of self-treatment we can do even without a proper diagnosis. I self-treated with over the counter antihistamines and quercetin (a natural mast-cell stabilizing bioflavanoid you can get over the counter) before I ever got a doctor to agree to prescribe anything else. Good luck!
Also, consider joining (for free) The Mastocytosis Society for support here: http://tmsforacure.org
They are a great help. (They are on Facebook too.)
Just freshly updated 2/22/21. Please try some of the formerly broken links again folks! Cheers. JG
What a fantastic job of pulling together this information. Have you heard of radio surgery / contrast or even non contrast MRIs causing mast cell reaction? I can no longer work since having a tumour zapped and experienced extreme reactions not seen by the medical team before. Very frustrating to not have answers! I’ve felt for a while that I have the trifecta and likely more! Had some result with Quercetin and antihistamines
Thanks! Glad you found my write up helpful. For sure, we are often sensitive to contrast dyes in scanning, but I haven’t heard about reacting to radio surgery (I’ve never heard of it before now), or non-contrast MRI reactions. That doesn’t mean they can’t happen!
We are often allergice to bee and wasp venom (stings), which translates to allergy to iodine contrast dye (first-hand experience here). But we can also be sensitive to EMF radiation so I don’t know if that would apply or lend a clue?
I’ll just say this much, if anyone can react to something odd or unusual, it is us! So if you feel you are reacting to X or Y, you probably are. Trust your gut (and body) always. This post may help: https://ohtwist.com/finding-your-mcad-triggers
Cheers.
Your description sounds so much like one of my diagnosis – vestibular migraine with brain stem aura. I also have EDS, PCOS, RA, hypothyroid, BP issues and others. But the mast cell thing sounds so much like VM. I can see I’m gonna head down a whole new rabbit hole with this one. Researching this angle sounds way better than that lumbar punctures regimen my neurologist is offering. Thanks!
Somehow that doesn’t surprise me. 😉 Our (over-active) mast cells are responsible for wreaking all kinds of havoc in our bodies, and this includes migraines, as these articles note:
The role of mast cells in migraine pathophysiology 2005 Theoharides, T https://pubmed.ncbi.nlm.nih.gov/15960987/
Roads Less Travelled: Sexual Dimorphism and Mast Cell Contributions to Migraine Pathology, Loewendorf, Matynia et al 2016 https://www.frontiersin.org/articles/10.3389/fimmu.2016.00140/full
Be sure to grab a snack before tumbling down that very long rabbit hole, indeed. 😉 Cheers.