Depression and EDS and MCAD

I really need to include anxiety in this post as well, as the two – depression and anxiety – seem to go very hand-in-hand for a large number of us. No surprise, this is true for the commonly comorbid autism spectrum as well, coincidentally. Maybe we’re finally onto some of the underlying organic causes of our anxiety and depression, as I hope to share below. Fasten your seat-belts and settle in, it’s quite a ride.
I’ve seen every variation on a theme of depression, anxiety, bipolar, mixed mood disorders and personality disorders of every kind really quite commonly in our groups along with all variations of ADD and OCD, even if some don’t recognize it fully in themselves yet. (Especially Narcissistic Personality Disorder, who tend to not want to recognize anything in themselves but nitpick on others.)
But quite a few have been diagnosed and do, myself included. I suffered from seemingly intractable depression and mixed mood disorder (aka “dysthymia“) off and on for years – until recently! (So did my late parents in various forms, underlying their alcoholism.)
Now gee, why, when my body has fallen completely apart in the last few years starting at 45, I stopped being able to walk and dance freely and live in unending and often severe amounts of pain would I feel less depressed than I ever have before?
Yes, it’s partly because I finally have some answers for it and the validation that comes with that. This has been huge. (Finally, it’s not all in my head! I’m not “just depressed” or my fav: “just a woman”, heh.) But I assure you, that is not the whole picture. (Though it’s definitely not trivial!)
I most definitely did suffer from primary organic dysthymic depression in the past, but really don’t any more. And I now think I know why. The good news here, is that if you do suffer from depression or anxiety (including panic disorder) and EDS, you’re definitely not alone!
The even better news here is, there’s a lot more that you can do about it besides just taking SSRIs like Prozac! (If you benefit from Prozac etc., do not apologize or stop taking it. This is aimed at those who got little to no benefit from it and other SSRIs for reason I’ll be explaining below.) And some of these solutions are free or very low-cost (over-the-counter). How cool is that? I’ve never been more hopeful in my life – for all of us!
NB Do NOT, repeat not stop taking any medications, especially antidepressants without the advice and supervision of your doctor, no matter what you read here or anywhere else. Many antidepressants require very careful, supervised and SLOW stepping-down to come off safely, and, some of us will still need them, even with all the tips I’ll share below.
(Please listen to Dr. Kelly Brogan explain why here! Or read about some here too.) Okay, ’nuff with the caveats! What have I learned that’s helped and how?
As I fell down the Ehlers-Danlos Syndrome rabbithole after my sudden disabling and upending onset “storm” or cascade in early 2012, I soon learned that hypermobility has been correlated with larger amygdalas, the emotional “fight or flight” seat of the brain. Gee, could this be why I’m more emotional on average and easily scared than some of my peers in general?
They also rightly noted in that study that comorbid dysautonomia can lend to anxiety also. And anecdotally most if not all of us are either on or related to someone on the autism spectrum where I’m finding anxiety truly quite rampant and sometimes show-stopping.
I soon learned about comorbid Mast Cell Activation Diseases (MCAD) of all kinds (Masto and MCAS) after @Mastocytosis followed me on Twitter in 2012 too, and realized most if not all of us seemed to share some form of this too. Boy has this explained another large portion of my life experiences – IBS, headaches, easy flushing, itching, hives, vomiting, bad reactions to anesthetics and iodine contrast dye and bees, the penicillin (mold-based) class of antibiotics, and much more. (Hold that thought. Yes, this looks a lot like – and may include – histamine intolerance.)
Turns out I’ve been going mildly anaphylactic all my life, but didn’t know it ! And had been getting dismissed as being “just sensitive”. Well! Now I know why! And suddenly I could start getting a handle on some of it by identifying and removing many food and other triggers, even as I found myself increasingly reactive as I entered peri-menopause. Turns out this is a common experience we find likely hormonally driven, and many women end up getting their MCAD (and/or EDS, especially Hypermobile type EDS) diagnosed around this time in their lives now, no surprise! Good news ladies: it gets better for most post menopause.
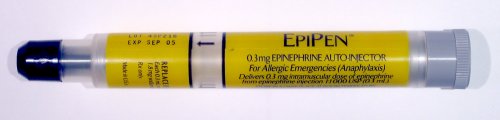
And what do you know, but anaphylaxis often includes a “sense of impending doom”. Uhm, gee, I don’t suppose this could possibly be driving any panic attacks by any chance now do you think? And no, I don’t just mean the highest level, Stage IV epi-pen requiring “ana” that is the only level most doctors, nurses and EMTs recognize currently, but some of the lower grades as well. What? You didn’t know anaphylaxis comes in grades? (Google “grades of anaphylaxis” and you’ll find more tables to choose from.)
Well join the rather large club who don’t. Because it sure does, and I now realize I’ve been living in the lowest “Grade I” semi-permanently my whole life, with regular (almost daily) dips into Stage II and occasional dips into III with a rare taste of IV on occasion.
I’ve determined that I’m what we call a “lucky leaker”, meaning I don’t usually go into full shock quickly and hard like some of my less fortunate colleagues who we call “shockers” who have to epi a lot more often. My mast cells just “leak” some mediators, vs fully degranulating – usually.
So I experience all the same signs and symptoms of shockers, just much more slowly and thus more mildly on average, making it extremely hard to recognize as what most doctors consider “true” anaphylaxis, which is a faster reaction that lands you in Stage III – IV quickly, requiring medical attention and often the use of epinephrine. I can change this by increasing my stress and trigger loads, and or being stung by a bee, smile.
We all carry epi-pens or should, anyway, though I’ve been able to keep mine buried for years (knock wood quick). Some of my friends epi daily – how they manage this both physically and financially I’ll never know, but they do because they have to. I do find the calmer I remain, the better I fare, and my friends have found the same. But every body is different, and you do what you must to properly manage with your doctor’s guidance.
It soon became clear to me that the comorbid dysautonomia (including POTS) and all that it entails is likely the love-child of both weak connective tissues lending to poor circulation and venous tone from flaccid veins and weak valves, along with hypovolemia (decreased blood volume) from a combo of stretchy bladders that can overfill and make us pee too much out, and the effects of mast cell mediators driving vasodilation and third-spacing and frequent urination. Low BP and sudden drops, lightheaded or dizzy, anyone?
Keep your fluid intake up – but with sufficient electrolytes to make it stick. Many find plain water to just go right through us – try coconut or Smart Water (or make your own), instead.
I also just learned a majority of us show signs of low magnesium levels. This is true for virtually all Americans, where our soils have been too depleted by modern industrial ag techniques, no matter how healthy we eat. But for some reason this is even more true in Ehlers-Danlos patients. Possibly due to our weaker epithelial layers and likely leaky guts lending to malabsorption and malnutrition even in the “healthiest” of eaters among us. I just learned this can lend to our electrolyte imbalances which lends to fluid imbalance also. Get your magnesium up any way you can so you can keep hydrated!
I also always have to pee like a racehorse after a reaction (lowering my fluid levels further), which is just about every other day presently. I’m trying hard to reduce this, but so far no dice. It’s a bit like taking diuretics all the time unintentionally and needlessly. (I.e. against medical advice!) But all I’ve done is eat and drink and encounter scents, stress and vibration while living my normal life. Low blood volume and pressure, here we come.
Toss in some neurogenic trouble from often occult Chiari malformation and Cranio-Cervical Settling and Instability (CCI) from weak neck ligaments and saggy hind brains, and impinged vagus nerves and I think I’ve got your BP drops and tachycardia and (some) sudden vomiting and tachycardia explained now. Uhm, I don’t see any reason at all to be anxious now do you? <sarcasm>.
And again, it’s not that you’re just scared or nervous about what’s going on, it’s that your body is literally having a physiologic reaction to physical stimuli (low blood volume, neuropathy, low BP, high histamine) that makes you feel like you’re anxious and can make you so, since you don’t seem to have control over it at times. Combine that with possibly less developed frontal lobes in some of us, and those oversized amygdalas and saggy hind brains lending to Sensory Processing Disorder, and of course we’re prone to catastrophic thinking, overwhelm and panic attacks! I defy you not to be in our case.
So along with baseline higher levels of anxiety on average, we “enjoy” plenty of episodic anxiety attacks thanks to our (often milder) MCAD reactions that doctors rarely recognize for what they really are: mild (and sometimes more severe) anaphylaxis and hypovolemic shock on top of occasional true and serious connective tissue injury and dysautonomia from Ehlers-Danlos Syndrome. But no, we’re “just anxious” they all say. Sigh.
But I digress. Where does the depression come from you rightly ask? I’ll tell you. There is increasing evidence that much depression is driven by neuroinflammation, which Dr. Theoharis Theoharides has tied to mast cell activation in the brain. So what are mast cells?
Mast cells are part of our primary immune defense system, the “first-responders” in the body if you will to invaders like bacteria and viruses and… innocent peanut and other proteins (aka allergens or triggers) when our immune systems are dysregulated and over-reactive. They are a form of white blood cell born in our bone marrow, but are kicked out while young and undifferentiated.
They then quickly migrate out of the blood and into all of our external facing tissues: skin, lungs, GI tract lining, nose, ears. You should have very few/no mast cells in your blood on average, they don’t stay there. Talk to a hematologist if you do.
They contain granules filled with many “mediators” or chemicals and proteins they release when triggered to varying degrees. They also make some on the spot during reactions too. But, and this is key: they also line our blood vessels, nerves and are even in the brain lining the hypothalamus!
 And guess what the hypothalamus drives? The pituitary-adrenal (HPA) axis! Uhm, hyperadrenergia anyone? Trouble falling and staying asleep? High arousal? Weepy? Moody? Check your histamine levels, you’re probably enjoying histadelia. I like to say I’m “Type A” for “Adrenergia” now. Or was, I’m doing a little better since catching on and managing my reactions more.
And guess what the hypothalamus drives? The pituitary-adrenal (HPA) axis! Uhm, hyperadrenergia anyone? Trouble falling and staying asleep? High arousal? Weepy? Moody? Check your histamine levels, you’re probably enjoying histadelia. I like to say I’m “Type A” for “Adrenergia” now. Or was, I’m doing a little better since catching on and managing my reactions more.
Toss in any undermethylation driven by MTHFR and company which run in up to 40% of the population (or more), and it’s only amplified, whee. Bipolar anyone? Are you sure?? Maybe you’re just eating wrong for your body type, no kidding. Get enough dark green leafy veggies or some methylated B12 and you may be a whole new person.
“True” allergies involve the triggering of IgE receptors on our mast cells which an allergist can detect and test for. The IgE has a “memory” for a specific protein it has encountered before, and is primed to react swiftly and more severely, often leading to full medically recognized Stage III-IV anaphylaxis from full mast cell degranulation. Carry those epi-pens and use them as directed if needed folks!
So technically you can’t have a true allergic reaction (involving measurable IgE) the first time you encounter a food or trigger – it has to engage the secondary immune system and generate those IgE memory antibodies over hours and days that then stick to your mast cells waiting for any more peanut protein or grass pollen to come wafting along before they trip out. Now that second or third time, watch out! They’re primed and ready to go, and how!
But with MCAD, we still do not know the direct physiological triggering mechanism of the mast cell yet (i.e, what’s the receptor? how triggered?), but it can happen both the first time you encounter something, and respond to non-protein triggers like heat, cold, vibration, pressure, scents, sunlight and sounds. Yes, tricky! And understandably a bit hard for doctors and even our own families and friends to believe. (Why I don’t go out much anymore.)
And in a further plot to confuse, you can suddenly start reacting to something you’ve always been able to handle or consume your entire prior life for no apparent reason! Yes, crazymaking!! Check your stress levels, and monitor your hormones, these may be playing a role. I always wanted to be a detective, little did I know I’d have to play one every single day for myself one day. (Now what did I do/feel/eat/drink/experience to cause this latest reaction?)
Mastocytosis involves having too many mast cells usually in clusters or clumps throughout the body, sometimes on the skin (urticaria pigmentosa, TMEP) that are almost always also over active and make you sick like you’re constantly allergic but without having “true” allergies you can test for. (Allergists regularly call us crazy and kick us out of their offices.)
Mixed organic brain syndrome has been correlated with systemic mastoyctosis since 1986. Then we slowly started recognizing its sister disorder, the new diagnosis on the block: Mast Cell Activation Syndrome, which you diagnose in the patient who is symptomatic like they have mastocytosis, but negative for signs of excess mast cells. (Ours are just “Type A” over-achievers, sigh.) But the net effect is still the same: you may still enjoy signs of mixed organic brain syndrome just the same. It’s just harder to diagnose the underlying disease driving this!
Though they appear to be catching on now. The Low Histamine Chef thankfully noticed this back in 2014 also as she discovered the connections Dr. Theoharides was making. Toss in the continued observations being made about the prevalence of psychiatric disorders in the hypermobile patient and is it any wonder we seem to enjoy just about every form of mood and psychiatric disorder known?
And The Sessions with Sean Croxton just shared a fantastic in depth interview with the brilliant Kelly Brogan, MD who has a book coming out about this very thing soon (next week, as I write this update March 11, 2016.)
But stop the presses! That means we can do something about it! In the case of our mast cells, we can both avoid known triggers (once identified, and this can be really tricky and take a bit of sleuthing and lots of patience and discipline), and reduce our reaction levels through the use of mast cell stabilizers like quercetin and luteolin and cromolyn sodium. And we can ease the histamine effects with antihistamines. (Those of you with true masto may need to address your proliferation with the help of a hematologist/oncologist.) And lowering stress which may be one of the biggest triggers of all as per The RCCX Theory by Sharon Meglathery shared February 2016.
But what about my neurology – aka funky brain shape – you well ask? Aren’t I just born this way and stuck with it? Not at all! It can take a while, but just as we can shape our bodies with “body building” exercises, so too can we re-shape our brains to a great degree with intellectual exercises and brain training, no kidding!
Dr. Robert Melillo even thinks all ADD stems from imbalanced brains, where one side is larger than the other, or the two sides aren’t “talking” to each other well. You can read all about this – and his great therapeutic solutions for it in his book Disconnected Kids. (I’m increasingly albeit unscientifically convinced that hypermobility lends to these imbalanced brain shapes and neurologies – whence all the SPD, OCD, ADD etc. we “enjoy”. But we need to study this!)
Many including myself will benefit from various forms of Cognitive Behavioral Therapy, including Dialectical Behavioral Therapy in particular. Does this take work? Sure. But aren’t you worth it? I can tell you it did a lot for me, even prior to changing my diet and lowering my inflammation levels in recent years. As well as from “tapping”, aka Emotional Freedom Technique as described here, which can help with all kinds of issues including anxiety, pain and focus.
And everyone can benefit from the simple practices of mindfulness and meditation, even for just a short duration, as little as 15 minutes a day. Just put away or turn off all your screens and electronics so you are not distracted, and settle your focus and attention on your self, your surroundings and your internal world. Observe and notice the world around and inside of you. Observe your breath. Even just breathing in through your nose and out through your mouth is shown to calm anxiety. Further, you cannot hyperventilate that way: it’s physically impossible.
The Low Histamine Chef Yasmina Ykelenstam has overcome much of her anaphylaxis through mindfulness practice and yoga alone, along with her nutrient dense diet.
I never did better than since going on a full reverse elimination diet in 2013 (I essentially did the GAPS diet, going down to chicken broth for 3 days before slowly adding foods back in one at a time only one every 3 days). This immediately and dramatically lowered my unrecognized (by me!) inflammation levels. My pain lowered, sleep improved, brain fog cleared, strength improved, IBS reduced. While I wasn’t able to sustain this indefinitely, I’ve remained on a diet I find best for me: grain-free high fat and protein, with plenty of kale/apple/kiwi juice when I can make it. (I’m lucky, I can eat kale.)
But every body is different, and you need to find the diet that works for your body and metabolic type ultimately. It may be different than mine. But just doing this alone can greatly reduce your pain and inflammation and neuroinflammation enough that you may calm many of your reactions and resulting symptoms and issues.
The large MCAD groups on Facebook are full of stories of kids (and adults) regaining speech on quercetin and luteolin. Conversely, many complain of losing their speech (apraxia) during reactions. No surprise, Dr. Theoharides has linked MCAD to autism as of 2015.
The groups are also full of stories of wild mood swings and melt downs at the start of anaphylactic reactions. Many seem to calm upon taking some Benadryl. I’m finally recognizing this to be an early sign of anaphylaxis in myself. It only took me 48 years! But better late than never. I’m not losing my mind – just my body!
And maybe you are too. I hope this has helped give you some hope for recovering from some mood and depressive disorders as well as easing anxiety attacks and anaphylaxis. Yes, what a long strange trip it’s been. But, at least I’m finally getting some answers, and now hopefully you are too! And again, you know that you’re not alone in this mental health journey. To those who may be judging us, know that MCAS is much more common than you think – possibly in as high as 14% or more of the population per some recent papers I’ve read. (I need to dig up that source still, but it’s late so you’ll have to wait just now.)
Let me know you’re experiences with all of the above in the comments. I think we’re starting to circle the same drain or hill as the autism community in terms of recovery answers, personally. I’m willing to bet we’ll be correlating hypermobility and autism all too soon, along with MCAD.
Did you find this information useful at all? I can really use your support at any level here if so, TY! 
To your health,
Jan(droid) 3.0 2016

{kind=link}
Hello fellow blogger! I just wrote an MCAS post myself not long ago following my MCAS “diagnosis”. I am currently on a everything eliminated but rice, kale, Brussel sprouts, zucchini, Swiss chard, collards, quinoa, organic chicken and bison, maple syrup, agave and sea salt diet (all veggies cooked and all food frozen right after prep of course!)… Two days down, 28 more to go! 🙂 Just writing to say, I read you, I heard you and I appreciate you. Hope you have a happy day! 🙂 https://maymonde.wordpress.com/2016/01/18/mast-cell-activation-syndrome-mcas-on-leaky-pinatas-a-k-a-mast-cells-in-mcas/
Just read your great post on MCAS – love the “leaky pinata” analogy to explain MCAS! So true… though I wasn’t aware they leaked even in the absence of a trigger, so thanks for that. Yes, sadly it often becomes easier to list what we *can* eat vs what we can’t, though I do still encourage people to eat as wide a diet as they can tolerate to keep their nutrition up. And only organic, whole nutrient dense foods whenever possible. (See my last post: Trust – and heal – Your Gut).) Nice to “meet” you here! I’m pretty sure we’re in some of the same large online support groups if I had to guess. And glad your doctors are treating you even in the absence of positive confirmation testing.
Meanwhile, I think it’s great for people to realize there may be some very real, organic drivers of their depression and anxiety that are also treatable! But at the very least, explainable. I remember feeling very hopeless and at sea battling my depression years ago with little help from SSRIs. Now I know why! And I’ve never felt better- at least emotionally, ironically. Cheers!
I learned a lot from this post. I didn’t know there were levels to anaphylaxis, wow! I’ve recently been diagnosed with MCAS, so I’m trying to learn all I can. I feel I’m right there with you having mild anaphylaxis since I was 22, and began using Benadryl for the beginning of the attacks. My next thing is to try the diets you mention. I’ve heard of them before.
So glad to hear it was helpful! That’s why I wrote it – to help others connect more dots and empower themselves with this information. I hope you continue to find more remedies that work for you accordingly. I’ve sure found it helpful to know! Good luck.
I forgot to add EFT aka “tapping” as a remedy above until today (just added it). It’s great for much of what ails us, but especially anxiety. It’s free and pretty easy and highly effective per most who’ve tried. Here’s one teacher (no affiliation or kickback):
http://www.emofree.com/
Here’s another: http://www.thetappingsolution.com/
I have been doing EMDR and tapping. It’s been going well so far. ?
Yay, I’m so glad to hear that! May your success only continue!
I also very much recommend Complex PTSD: From Surviving to Thriving by Pete Walker. The more I read, the more it seems like BOTH psychological stress and trauma could cause our myriad physical issues AND vice versa! It’s impressive, really.
Thanks for the great recommendation – I do think CPTSD is also common among us (I see it a lot anyway, and think I experienced some myself). Will defo try to check that book out. I do agree the two issues (physio vs psycho-logical) go hand in hand and can drive each other. A lot of our most afflicted patients have experienced trauma from childhood or later. (Myself included.)
You’re welcome! And definitely — my one minor quibble with his book is that he barely mentions the possible physical ramifications, and doesn’t mention the possible truly severe issues when he talks about hypochondria (from chronic anxiety from trauma). But it’s understandable, as he’s a therapist, not an MD, and hasn’t experienced severe health issues himself, as far as I can tell. Oh, this is the article that was my first introduction to his work — but warning, it made me cry quite a bit. Having an easier time with the book, not sure if that’s because I’ve been thinking about this for longer now, or what. https://www.psychotherapy.net/article/complex-ptsd
Oh, and I think you’d be really interested in his theories about how things like ADD, OCD, BPD, and NPD can relate to C-PTSD! Especially with the bit I just read of your post about autism and EDS.
Thanks – I’ll definitely check his book out!
I’ll be editing the above post to add a little emphasis for women on the potential effects of oral birth control lending to depression also thanks to a passing comment someone made in one of my support groups recently. The light bulb went off for me, and I recognized that I did get distinctly less depressed after I switched from a triphasic OBC pill in 2001 to a steady progesterone only pill to suppress my periods – at that time, just for convenience. All at the suggestion of my OB GYN at the time who noticed I was about to travel overseas and asked if I’d like to avoid my period on the trip. (The timing was just right, by coincidence.)
So I did, and along with no longer menstruating for the next 6 years, my mood was elevated. But it was just subtle enough I didn’t associate it with stopping the triphasic pill. I just assumed I had somehow gained wisdom and insight with age and was just slowly naturally growing out of it (blessedly and thankfully after too many years of really dark thought spirals).
Then I stopped taking all birth control altogether at the suggestion of my LAc in 2007, and have never felt better, even including since becoming disabled. How could that be? Well, rebalancing my own natural hormones and detoxing from the other may just be part of the picture as Dr. Kelly Brogan notes here:
http://kellybroganmd.com/that-naughty-little-pill-birth-control/
And more fuel for my views about inflammation driving depression above:
https://www.ncbi.nlm.nih.gov/pubmed/28418288
Hi Jan, re inflammation – are mainstream blood tests reliable in determining the level of inflammation?
I thought I’d have some but my bloods said otherwise. Thanks, Zel.
Great question, and I’m not entirely sure. Like, yes, gross inflammation should be picked up in things like elevated CRP, but I’m not sure that low-level chronic inflammation from things like MCAS can be “detected” in blood outside of elevated histamine levels, usually measured in urine N-methylhistamine, a metabolite of histamine. I would try for a 24-hour catch vs spot check if can.
The real test for me? Reducing/removing as many known “triggers” for me as possible, and seeing how I feel/fare. Boom – almost always much better, including elevated mood. Conversely, I get a really dark mood swing during almost all of my MCAS reactions. Like, from zero to nearly suicidal in under an hour. I’m constantly talking myself back off of various (invisible) ledges. (Yes, it’s exhausting.) HTH.