On Variable Expression
From the online Genetics Home Reference, variable expression is defined as:
“Variation in clinical features (type and severity) of a genetic disorder between individuals with the same gene alteration, even within the same family” [italics mine, JG]
Definition from: GeneReviews from the University of Washington and the National Center for Biotechnology Information
Take the trait for red hair for example. Even if multiple members have the same genotype (genetic trait, allele or DNA for red hair if you will), one may have a somewhat lighter or darker shade (also known as “phenotype”, or outwardly visible physical expression despite genotype) than the other. The same can hold for any other trait we inherit, including hypermobility (or “bendiness”) for example. And when you toss in innumerable other possible mutations you may have along with a particular EDS defect or “SNP” (single-nucleotide polymorphism – a fancy word for mutation or alteration from the “norm” or “wild-type” occurring in the majority), it’s no wonder no two people with EDS present alike even in the same family with the same genetic collagen trait. Toss in epi-genetics, or factors that affect the expression of DNA (activating some bits, shutting down others, some helpful, some harmful), and it’s no surprise that not only are we not alike, we experience our EDS very differently, despite some common themes. (This is even true for twins). When you consider the numerous systems we’re finding to be affected by faulty collagen as I’ve already described, and is it any surprise doctors miss diagnosing EDS when we present with everything from mood disorders to fallen arches, allergies, hemorrhoids and myopia? I now believe all doctors have seen EDS patients, whether they know it or not.
But until someone points out the common collagen thread running through all of these issues, some of which are only recently coming to light as commonly comorbid such as the mood disorders, autism spectrum and digestive problems and atopy (allergies), there’s no reason a doctor would logically suspect EDS. Especially not when they’ve been told it’s rare, and only given some of the most extreme and externally visible signs to suspect it with like stretchy skin, full dislocations and odd scars. Why would they ever suspect the mildly (or more) anxious or depressed but smart woman presenting with myopia, hemorrhoids and generalized joint or back pain or fibroymyagia that can’t be diagnosed with the usual scans? They’re so much more likely to write us off as just depressed and anxious, which we may well actually also be (I once was), but yet still definitely suffering physically, even if not visibly yet. (If only pain glowed!) And women are disproportionately affected from likely hormonal influences (progesterone makes you more lax, and estrogen heightens mast cell activity), although it runs equally in both sexes as far as we know. (It is not an X-linked trait).
Ehlers-Danlos Syndrome can also be “triggered” by sickness, stress and trauma, such as the death of a loved one or a car accident or nasty flu, and this also adds to the confusion. Much like with CFS/ME, a patient may only remember getting sick, and just never getting well again, or not very. Others will have no major issues or illness or trauma, but have a slow and steady stream of joint problems and tendonitis and cartilage loss that gets written off to just “wear and tear” or age, since we’re often so driven we work in very physically demanding occupations and such trouble seems to be the “norm”. (E.g. bad backs, fallen arches and bad knees in cashiers or warehouse workers). Others will have few joint problems, but really struggle with the “extra-articular” (non-joint related) problems I’ve mentioned elsewhere and below.

You could say we put the “variable” in variable expression (smile), with such a wide range of resulting comorbidities and variable presentation at any and all ages and rates of onset. Babies, can’t talk, but they can be floppier than “normal” (aka “hypotonic”), and be slow to walk and or talk, W-sit, and have lots of allergies or bilateral hip dysplasia (dislocations/displacement on both sides). Toddlers can likewise struggle with coordination and strength, fatigue easily, cry from pain, melt down easily from sensory processing disorders (SPD) on top of internal pain, etc. Older children may have trouble with constipation and/or diarrhea, or even incontinence from allergies and MCAD, tethered cord syndrome or occult Chiari, plus extreme lordosis (inward curvature of the lower back, aka “swayback”), scoliosis or hernias. Children may walk with an inward toeing gate that needs to be corrected before it’s “set” in them, have a pronation or flat feet, or require orthotics like AFO’s and KAFO’s to support weak ankles and knees. They may have trouble falling and staying asleep, and do better with a small snack before bed, especially protein and be prone to headaches and “tummy aches”. (One friend’s daughter was so “floppy” she had to cover her in braces from nearly head to toe).
Both children and adults may have trouble regulating temperature (get hot or cold easily), pass out from low BP easily especially upon standing quickly or for too long, have exercise intolerance and mood disorders including irritability from SPD and histadelia from likely MCAD and atopy (allergies). Most will have a long (and ever-growing) list of food and drug allergies and sensitivities, be allergic to bee and wasp stings, flush easily, experience hives and other odd rashes and skin issues.
Children and adults my find themselves prone to chronic or recurrent infections, often ear, sinus and respiratory infections as children, and UTI’s in adults. Scarlet fever is not uncommon, along with proclivity to catching just about any virus that comes along no matter how careful, including STDs. (This may be a result of likely CVID and variants we’re finding common in the community). Yeast infections and thrush are common, as is Small Intestinal Bacterial Overgrowth (SIBO), low stomach acid, and weak hiatal sphincters and ileo-cecal valves. (That’s the one between your small and large intestines that keeps things from flowing back up your digetsive system). Appendicitis and gall stones and other gall bladder trouble are common, along with vocal cord dysfunction, asthma and early or noticeable hair loss in women.
Hernias, prolapses, tendonitis, bursitis and cartilage loss set in with age, as early as the teens and 20’s in some poor souls. Osteopeonia and early onset osteoporosis are also common. Cracked or weak teeth are also common, along with receding gums and the need for partial or full dentures even at relatively young ages. (My mother had full dentures by the time she was 36).
We also seem prone to aneurysms, significant aortic root dilation and mitral valve prolapse even at young ages, some as young as 5. (I know, I’ve met the record-breaking sweet medical conundrum named Stryder myself. Doctors are still trying to figure him out!) We’re also finding epilepsy and all types of seizure disorders somewhat common, as well as MS like symptoms and issues. Also signs of electrolyte and nutritional deficiencies and imbalances (especially potassium, Vit B12 and Vit D), kidney dysfunction (including diabetes insipidus, not just mellitus) and fibromuscular dysplasia (deformity of the arteries, especially renal ones, including aneurysms).
And lastly, I see a LOT of people on the autism spectrum in our community, either patients themselves, or family members, such that I now personally suspect anyone who is. (This is just a personal theory as yet, but I would love to see it validated by a serious study soon!) We certainly experience a lot of depressive and anxiety disorders which I now believe to be organic and / or secondary in origin, and often improved with allergy-elimination and CBT. Many EDS families have members who exhibit Narcissistic Personality Disorder (NPD), as well as OCD and ADHD. We’re all often high achievers, very driven and bright, though learning disorders like ADHD and dyslexia are not uncommon either. Many get diagnosed with the “alphabet soup” that seems to go with those who don’t meet the threshold for a diagnosis of actual autism spectrum disorders, whichever version of the DSM or standard you are using. (ADD, ADHD, OCD, PDD-NOS, etc.) Many are very stubborn or impatient, not suffering fools gladly so to speak. A lot show signs of codependency (being overly-solicitous, indecisive), possibly in response to living with a narcissistic parent who demands their needs be met first in all cases, as I did.
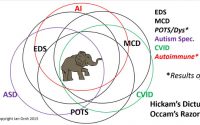
Like I’ve said, it’s more like sixty blind men and an elephant than just six. (Oh to have just six!) Is it no wonder we’re missed and dismissed as hypochondriacs or Munchausen patients, as we are shuffled from one specialist to another including psychiatrists, podiatrists and therapists, with few primary care doctors noticing that common collagen thread running throughout all our issues? Obviously not ALL people with any of the above issues individually may have EDS, nor will, but, if you notice a large number of them comorbidly (existing together in the same person), it should sure lead you to suspect them further! My personal term for the subclinical EDS patient is the “Walking Wounded”, and there sure are a lot of them! If I can do nothing else but help raise awareness of the subclinical presentation of EDS and its increasing prevalence, I will die happy.
Off to take a rat nap with my Chief Napping Officer Peanut,
Jan(droid) 3.0 better, faster, stronger! One day (and nap) at a time…