When Else to Suspect Ehlers-Danlos Syndrome
This page last updated December 22, 2024, originally posted in 2017.
Prior to March 15, 2017 we spoke of six main forms of EDS only, and some additional hypermobility syndromes (HMS, JHS, BJHS) which seemed to share a lot of overlap and confused everyone.
These have all been folded into either the newly sharpened EDS criteria, or the new categories of Hypermobility Spectrum Disorders for those who don’t meet the tightened diagnostic criteria for hEDS (the most common form of EDS by far) as of March 15, 2017 for any reason but exhibit a lot of the following issues just the same, indicating some kind of systemic connective tissue disorder, after all clear ones have been excluded. (E.g. OI, Marfan, Stickler, etc.)
The more rare forms of the Ehlers-Danlos syndromes are usually enough easier to suspect and diagnose (generally) due to their severity and/or distinct signs that they generally have less trouble doing so. But do be sure to do very proper full differential diagnosis if suspecting any form of EDS or HSD.
Please consult The Ehlers-Danlos Society for more information on all forms (March 2017).
Original post March 2017:
I wrote about my top five ways to suspect hypermobile Ehlers-Danlos Syndrome a couple of years ago. These included:
- Fibromyalgia
- IBS
- Chronic Pain
- Anxiety, depression and Autism Spectrum (and ADHD now, 2021)
- Allergies and sensitivities or MCAS (a form of MCD)
But I keep finding so many additional common signs and symptoms that people exhibit, that I felt them worthy of another post so am hatching this one.
Though let me be clear, many of these are actually common comorbidities still, and none of them is truly diagnostic alone. Just part of the trail of breadcrumbs I hope you find leading you to suspect and look further into connective tissue disorders (CTDs) including the newly recognized most common Hypermobility Spectrum Disorders, as well as the more rare forms of EDS and other CTDs like Marfan Syndrome, Sticklers, Loeys-Dietz and OI.
(If you do suspect one of these conditions, check out my Diagnosing EDS and HSD page for some tips on going about it with your doctors and start gathering family history to that end.)
However, rather than expounding on the signs I’ll just list them with a few links where able to outside sources about them.
Again, because this is a systemic condition the myriad ways it manifests are rather mind-boggling in number and ultimately limitless: they affect the whole body in some way or another. This seems to be what makes it so hard for doctors to identify the condition prompting some wise anonymous person to quip:
If you can’t connect the issues, think connective tissues – author unknown*
*If you know the author, please tell me so I can give proper credit! And no it’s not Dr. Heidi Collins – she said she doesn’t know either. She just quoted them too! (She says so in her 2014 talk of the same title at the EDNF Conference, no longer available on YouTube as of 2024.)

The thing is, most doctors have only been told about or possibly only remember the grossest signs of the rarest types (of EDS and all HDCTs) for the most part, so many of us with less hypermobile or gross types keep getting missed still. Why I’m writing!
Anyway, on with the unofficial and incomplete list. And if you find yourself checking off more than not, I would highly suspect you of some form of connective tissue disorder!
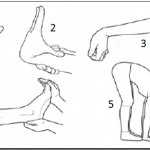
- Postive Gorlin’s sign (ability to touch tip of tongue to nose, yes I think this case has EDS, natch)
- Flying Bird Hand sign
- W-sitting (don’t do it!)
- Reverse Namaste or Namaskar sign (able to form the “Namaste” prayer pose with hands behind your back)
- Standing on the sides of your feet as your ankles roll easily in, or out – pronation, anti-pronation
- Severe myopia (near-sightedness) and or astigmatism
- Nystagmus or repetitive uncontrolled eye movements (magnesium may help)
- Chronic Blepharitis or eyelid infections (likely from Selective IgA deficiency, part of commonly comorbid CVID)
- Weak, crowded or cracked teeth (low Vitamin D contributes to the latter)
- Peg teeth, or abnormal shaped teeth or microdontia
- Receding gums that easily bleed even with good hygiene (Vitamin C can help this)
- Sensitive teeth – this can come on as your ligaments loosen. (Mine tightened up and the sensitivity resolved with Vitamin C therapy yay.)
- TMJ and all forms of jaw deformities, but especially high palate & crowding
- Stretchy skin, ability to flip eyelids up (and freak out younger siblings)
- Contortionist ability, or extreme flexibility in gymnastics or acrobatics
- Injure in your sleep easily. Have to adjust, reset or tape up joints upon waking and getting up. (Shoulders and hips go out easily if you side sleep. Also trouble sleeping on your back due to obstructive airway apnea from floppy tissues no matter your size.)
- Weak ankles, trouble wearing high heel shoes, strong pronation or anti-pronation
- Clumsiness and poor proprioception (sense of body location in space)
- Weak knees, loose patellas, hyper-extended knees
- Restless Leg Syndrome – some find magnesium to help ease this (not all)
- One side much weaker or more injury-prone than the other, not always your dominant side either
- Thin skin that tears easily and any scars that widen or grow or move
- Easily imprinted skin – we have semi-permanent “sock prints” or “underwear tattoos” imbedded in our skin in winter
- Fallen or falling arches, or any related issues (neuromas, plantar fasciitis)
- Walking with a strong pronation (ankles lean inward) or anti-pronation (outward). Trouble finding comfortable shoes that don’t alter the bone structures in your feet.
- Easy bruising
- Keratosis pilaris – tiny red bumps that show in patches on upper arms, buttocks and more
- Easy bleeding, trouble suturing, poor healing post surgery
- “Dodgy” easily blown veins, often require ports for infusions
- Any amount of CSF leaks anywhere along the dura, but especially out the nose or ears (yes, this happens! Suspect leaks if your headaches worsen the longer you are upright)
- Deviated septum
- Crossed eyes or wandering eyes from lax eye ligaments
- Bulging veins, varicose veins (especially early onset)
- Venous insufficiency
- Herniations or prolapses of any and all kinds including hemorrhoids
- Easy or frequent fainting or dizzy spells (likely from comorbid POTS and dysautonomia)
- Raynaud’s phenomenon or syndrome, livedo reticularis (purple “mottling” of skin) and all other forms of dysautonomia
- Chronic constipation with quick flips to diarrhea (IBS) – already mentioned in first post
- Lots of allergies of any kind
- Chemical sensitivity, multiple chemical sensitivity (likely really a form of MCAD)
- Insomnia and adrenal fatigue
- Sleep apnea, snoring, even in “thin” patients (weight doesn’t help, but we have weak laryngeal tissues), not to be confused with CNS apnea making you forget to breathe even in the daytime.
- Chronic headaches of almost any kind, including migraines
- Chronic idiopathic (unknown origin) nausea
- Bad handwriting, lax hand writing, trouble holding pens or pencils properly, need for pencil “grip”
- Chronic or recurrent infections, get sick easily or often fighting candida and viruses (likely from CVID or any other variations of primary immunodeficiency)
- Chronic or frequent heart palpitations or fluttering, tachycardia (PVCs and POTS are common in us)
- Chronic or frequent or multiple instances of tendonitis (aka tendinitis)
- Bursitis, chondromalacia of any kind (loss of cartilage between bones of a joint, any joint, though usually knees aka chondromalacia patella)
- Bone spurs (why this is true I don’t know, but they’re common in us)
- Spinal stenosis (narrowing of the spinal canal between the vertebrae, impinging your spinal cord sometimes)
- Easy flushing red (from MCAD)
- Trouble swallowing from floppy laryngeal tissues and CCI and mild/occult Chiari
- Hearing trouble from weak inner ear bones, weak tendons, or sensory processing disorder
- Sensory Processing Disorder of any kind (including lack of pain in some lucky cases)
- Poor temperature control (run hot or cold easily, usually cold) goes with dysautonomia
- Chronic fatigue (may be misdiagnosed as Chronic Fatigue Syndrome aka ME / CFIDS / SEID)
- Fibromyalgia (already mentioned, and very very common, usually an under-diagnosis for HEDS, may be worsened by comorbid occult MCAD of any kind too)
- EMF sensitivity – and tendency to “blow” nearby electronics
- Ganglion cysts, Baker’s cysts
- Petechiae
- Peizogenic papules
- Lipomas and lipedema causing unavoidable weight gain most often in women
- Osgood-Schlatter’s disease (knobby knees from rapid growth in childhood)
- Leaky gut syndrome, dysbiosis
- Hypochlorhydria or low stomach acid (unsure fully why, but it’s common and lends to dysbiosis and SIBO) – possibly from high cortisol and/or thyroid imbalance
- SIBO – Small Intestinal Bacterial Overgrowth (likely aggravated by weak ileo-cecal valves in us allowing more to “back up” than should plus low stomach acid as mentioned)
- Keratoconus (droopy or thin “pointy” corneas, hard to fit soft contacts)
- Sensitive eyes, trouble wearing contacts
- Weakness, mitochondrial disorders and disease
- Seizures, hypnic jerks, myoclonus and actual epilepsy
- PTSD, anxiety and panic disorders
- Depression and mixed mood disorders of all kinds
- Stretch marks or striae in any gender, not just after pregnancy in women
- Pelvic floor dysfunction, prolapses (uterine or rectal, bladder, any)
- Ptosis (drooping of anything, but most noticeably saggy breasts in women)
- Drooping upper eyelid or eyebrow sometimes requiring an upper eye brow “tuck”
- Sciatica
- Claw finger or hammer toe or claw toe
- Early onset arthritis of any kind, as well as any other auto-immune diseases (very common in us, likely secondary to leaky gut and chronic inflammation)
- Paradoxic reactions to medications, strong or strange reactions, need for increased novocaine or lidocaine
- Vocal cord dysfunction
- Trouble swallowing (can have both neurologic and allergy-type drivers)
I’m stopping here for now, but will periodically add to this list. Many of these were already listed on the common comorbidities page, but I’m trying to add signs that in themselves are not full comorbidities, but just signs we find common in EDS and HSD patients. Alas, I’ve caved and ended up adding/sharing a couple that are driven by one of our most common comorbidities I find: MCAD.
And I will re-iterate that though many patients are quite flexible or “bendy”, and some even extremely so, NOT ALL are very or even at all “bendy” or flexible! So do not consider yourself exempt just because you are not, sorry. Many of us stiffen with age and early onset arthritis, and some, like Dr. Jaime Bravo a leading rheumatologist in Chile with EDS himself told me never are in 2012.
Note March 16, 2017: They/you may now be getting re-classified as having a form of the new Hypermobility Spectrum Disorders instead of a form of EDS accordingly, but that remains to be seen. Check with your doctor using the new criteria guidelines from The Ehlers-Danlos Society please!



I have about 40 of these symptoms. The ones I don’t have, my family members DO have. This included my parents, sister, cousin, and 3 second cousins ages 3/7. I have CFS, POTS, hyper mobility syndrome, scoliosis, thyroid and adrenal weakness, TMJD. My GI dr believes I have gastroparesis. My mom has a brain anyurism, IC, CRPS, etc. I was told by a doctor I don’t fit the requirements for EDS… Yeah, I’m seeing a different specialist.
Good on you! Although I’m sorry to hear you’re a likely fellow EDS patient (and yes, quite likely from the sound of it), I’m glad I could empower you to advocate for yourself with your doctors with this post. One has to wonder just what else they think causes so many different issues in one body without thinking systemically. Good luck in your pursuit of a proper diagnosis.
Holy hell I have so many of these!!! And so do so many of my family members!! My son was diagnosed with masto, u.p. I had asked if things were connected; I have asthma, Ibs, skin conditions, tmj, plus my own allergies are crazy; they keep assuring me his condition was a fluke and not to care……I think I am going to mention this…..my mom has degenerative disc issues and a whole, laundry line of these symptoms, if not all of them…very interesting. Weird that none of us have been diagnosed with these….
Sorry you do share so many of these troubles and glad I could help you mmaybe connect some dots. Gather your family history as much as possible (not all can for a variety of reasons) and bring it to you docrors. I have a sample spreadsheet for same here:
http://ohtwist.com/about-eds/diagnosing-eds/
(You can adapt it or make your own of course it’s just a sample)
Good luck, Jan
Hi, sorry if this has already been covered – I only have the energy to read a few posts. I’ve seen Tarlov Cysts mentioned In connection with hEDS a few times. I’m wondering about other types of cysts like cystic acne, Skene duct cysts, Bartholins, poly cystic ovaries, fibrocystic breasts, all of which I have / had. I’ve just always wondered why I make so many cysts!
Boy, that’s a really great question! And I don’t recall seeing people complain of more cysts of all kinds in general yet no, but that doesn’t mean they don’t have them. PCOS is semi-commonly comorbid, too, yes. Have you recognized any signs of MCAS yet? I tend to think of MCAS when there are issues all throughout our connective tissues. It also causes adult acne onset in me during some reactions.
But bottom line I don’t know. I hope someone else chimes in on this.
Sadly, I have 4 of the top 5 (and previous had all 5). I (or family members) have so many of the long list it’s beyond my comprehension that I wasn’t diagnosed until my mid-40s and my mother died undiagnosed. Too bad more doctors aren’t familiar enough with EDS to put two and two together! We just end up suffering more and for much longer than necessary.
I’m so sorry you share my long painful journey to diagnosis – I too am the first in the family to be diagnosed, and only in my 40’s after falling completely apart from head to toe from a rare onset “storm” or “cascade” that left me extremely weakened all over. (I split my right SI joint, subluxed my R leg, fingers ribs and toes before it was done. I’m still dragging my R leg as we type 3 years later. I now suspect a progesterone “surge” based on subsequent monthly experience as a female.) Between my stubborn stoic family members “sucking it up” too much, and our poorly informed doctors “normalizing” the milder forms and failing to connect the isolated dots, no one figured it out until I suddenly became wheelchair bound in 2012 at 45. This is why I’m blogging – to help alleviate that for all of us, past and future… I pray others find this information and catch on so much sooner too! Glad you feel validated, but sorry you share my pain. Better luck to all of us!
My illness started as a ‘cascade’ too. It worked its way through my body. I’ve never heard anyone describe it like that before.
So sorry to hear that. My geneticist called it an onset “storm”, and then I heard Dr. Claire Francomano (one of the leading EDS savvy geneticists in the US) say they prefer the term “cascade” at the 2013 EDS Learning Conference I attended in Rhode Island. So I try to use that now too. Either way, sudden onsets are rare, but very real alas. Welcome to the club, sorry. Hope you are managing okay and getting some recovery and relief since.
This concept of a Storm or cascade and the role that progesterone plays was extraordinarily helpful to me. Thank you for sharing this part of your journey and for the awareness efforts! Although I have had some issues of one kind or another all my life, I was doing really well in my 40s….until all of a sudden I wasn’t. I’m almost 5 years into my body self destructing and yet the only reason I’m hearing of EDS is because my daughters podiatrist suggest to her that she has it and the two of us started comparing notes. Doctors need to think zebras!
Yes, they sure do need to “think zebras”! One day… Meanwhile, I’m so glad my story could help you to suspect a form of EDS or hypermobility spectrum disorder in yourself at least too. Let me add that the RCCX Hypothesis by Dr. Meglathery may also explain why so many of us also experience sudden onset “cascades” or storms (whichever) after a sudden truama such as a car accident, divorce or death in the family: if we have a borken hydroxylase 21 enzyme we may shunt excess CRH down a differnt pathway forming extra/more progesterone pre-cursor which may also lend to increased laxity, but is not as easily measured as the common form of progesterone. You can read all you like about that hypothesis here:
http://www.rccxandillness.com
That said, I’ve found staying as calm and happy as I can at all times to really help, and then being gentle with myself and my body when my hormones fluctuate monthly in spite of all my efforts to be most helpful so far. Good luck to you!
I’ve had a couple of doctors suspect I had EDS, without me even mentioning it to them. I had long suspected i might but didn’t feel I fit the flexibility guidelines so I dismissed it. But it kept coming up. I did my own DNA test and found a positive link to possibly having a form of EDS, but it’s not an official diagnosis. My father was adopted and I know nothing of this side of the family. But the one thing I have discovered in genealogy research is that the people I suspect to be his family all died so young, 60s-70s, from heart conditions. He died at 71. But I have yet to have a geneticist confirm my suspicion. The one RA I saw about this looked at me, yes LOOKED at me and said “oh you don’t have EDS, you don’t have that paper white skin.” Am I not translucent enough for you? So internally I feel I do have vEDS. I have so many health oddities that doctors can’t explain so they just want to give me a rx and “call me if you have any problems.” I do things holistically and follow a plant based diet and I feel like that has helped a lot with my symptoms. Thanks for jotting this blog.
Arrgh. You’re welcome. Cuz clearly we still have SO much more educating to do! Sigh. Sorry this is so. Glad to help you confirm some supsicions. Sorry you don’t have the family history to back it up – though, it sounds like you sort of do from your research.
Anyway, I will just keep pounding this drum and trying to lay out doctor scented bait on Twitter to get more to follow and learn from me and everyone else trying to raise medical awareness of this far from rare condition. Cheers.
Thank you so much for this! I have so many of these symptoms and recently had surgery for Chiari and cranio-cervical instability. Recently I saw a Rheumatologist who tried to discredit my diagnosis because he felt that I wasn’t “hypermobile enough.” It made me doubt my own diagnosis. I am 45 and have arthritis and have lost some of my hypermobility, but I have no doubt that my diagnosis is accurate. My mother is going to be accessed soon as well as my son.
So sorry to hear of another short-sighted rheumatologist – I find your experience all too common. I’m glad you found my page and info validating – I just wish I’d had known and been able to share this 10 years ago (or more) for all our sakes! Glad you got through your Chiari and CCI surgery okay – those are very tricky since we take longer to heal. But not at all uncommon. (I’m lucky to be a rare exception among my friends who are all going back east for the same 2 procedures plus tethered cord release one by one.) Good luck to you proceeding. And trust – and heal – your gut!
I have over 50 of these plus added major symptoms/conditions not listed on this extensive list. Thank you Jan for this list; given I am like many others turned away from dx due to rheumatologists negligence, I am needing to find out what other type of dr.s can diagnosis this? I’ve been told geneticists are the gold standard but I know my health insurance would most likely never cover this and if they did it would require a referral from another Dr. or specialist. I’m perplexed what type would be a wise choice? Also would like feedback to know what benefit would it be for an EDS / and or POTS, MCAD patient to get a definitive dx? I’m hearing there is no cure and not much as far as medication (most likely would have paradoxical reactions anyway) Are there certain anesthetic or other precautionary measures to take if you do have it. Are there supplements etc that can help slow down the rate of degenerative changes one gets as they age? I’m 52. Last question; Does anyone know if bladder, uterus, pessaries safe for prolapses?
I do think it’s worth diagnosing: this is the whole reason it took me falling completely apart at 45 to get diagnosed: no one does get diagnosed, so it’s thought to be rare. It needs to be recognized for as common as it really is, as it underlies oodles of other comorbidities, and treating it fundamentally (and being aware of it) can help prevent some secondary issues and injury. I.e, if a PT does not know you’re hypermobile, they can injure when treating for an ache or injury. Another friend increased her cranio-cervical instability by uknowingly riding a roller coaster. I have another friend who nearly broke her neck at a chiropractor’s because he used high velocity neck thrust techniques on her. (And he’s an Olympic team medic, so “knows it all”.) Plus, if you have one of the more severe forms like Vascular or Arthrochalasiac, it’s important for family planning and medical care and consideration. You need to be aware of both biomechanical (different or increased suturing and blood supplies may be needed), and biochemical issues going into any surgeries from the so commonly comorbid MCAD lending to anaphylaxis to anesthesias and medications.
And I would argue that there is too something you can do about it. I myself am benefiting from high dose Vitamin C plus cofactors (calcium, magnesium, zinc, potassium and Vit D plus a good probiotic); the Cusack Family is benefiting from this protocol she discovered (which I’m also trying to adopt when money allows):
http://ouredsjourney.weebly.com/
And the Facebook community is abuzz tonight with the news of a young woman “walking again” after being paralyzed from EDS after she got stem cell therapy in Mexico here:
http://www.chron.com/neighborhood/woodlands/news/article/Woodlands-teen-overcomes-rare-disease-to-walk-6715196.php
I of course second the notion to try seeing a geneticist, despite the hardship – many specialists won’t take a diagnosis from any other doctor seriously for some reason. I recommend rheumatologists second to that, but with the caution that most of them tend to find our comorbid and secondary autoimmune disorders first and stop there, ironically. This is partly why EDS goes so rarely diagnosed: it’s masked under the guise of so many comorbidities including MS, RA, Sjogren’s, Lupus, AS etc. (Many of which we do have as well.) That said, technically ANY doctor can diagnose EDS who is willing to read up on it and stick their neck out a touch. Just follow the guidance I give here: http://ohtwist.com/about-eds/diagnosing-eds/
Thanks for your blog, it makes very interesting readingto me, as i was ruled out of not having eds earlier this year by a rheumatologist, who told me that i was far too stiff to have it. She diagnosed osteoarthritis in my hands, shoulders, knees and so on. I have had pains in all these joints from being teenage. Over the years the pains come and go but, they have gone to more joints in my body, also tiredness resulting in low b12 from time to time. Twitching calf muscles that keep me awake at night. It all comes on in waves, one joint will ache, then leave and go somewhere else in my body. I know that i am not as bad as a lot of people but, it would be nice to make sense of it all.
I’m so sorry for this all too common experience with your rheumatologist. I can’t emphasize enough that you do not have to be “bendy” or flexible to be hypermobile and have EDS. Many either stiffen with age like myself (formerly super bendy, but no longer at 48 except in my fingertips, and some never are like Dr. Bravo himself). The Beighton 9 pt score really needs to go away, even Dr. Beighton agrees, and hopefully it might after next year’s international symposium in NYC in May 2016. This is the single biggest red herring we encounter that causes so many to be mis or under diagnosed still. And it’s misunderstood by both patients and doctors alike. Trust (and heal) your gut, and pursue a diagnosis with another doctor after getting well versed with the latest info when you feel up to it. Better luck!
Thanks Jan for posting this. I have over 50 of these symptoms on the list in addition to others not and was also told I wasn’t bendy enough, not even a consideration by yet another rheumatologist. I’m wondering how best to get this diagnosed once and for all given most people need a referral to see a geneticist; can’t afford one out of pocket. Been on disability for CFS and Fibro for years but have ALL these other symptoms and more to boot some which don’t necessarily overlap with CFS and Fibro though some do. I’m 52, not bendy anymore due to arthritis, severe scoliosis,DDD, SI joint dysfunction,severe knee issues, along w/ bladder prolapse, mitral valve prolapse, Heart arrhythmias, frequent low bld pressure and dizzy (used to faint regularly as a child) bleeding disorder platelets aren’t many ones that I have don’t respond to clotting factors well with history of major issues not just frequent bruising, vocal chord dysfunction + 2 other vocal chord dxs, apnea (i’m extremely thin) frequent tenosynovitis in wrists and fingers, and recently a worsening ankle pain that prevents me from being able to walk many days a week. No rheumatologist can answer why I have trouble walking and just say its that I’m getting older, must be from fibro. Any ideas from anyone how best to find a dr? would it be a neurologist? I also can’t have certain anesthesics due to a genetic disorder that runs in my family that I just found out about( was adopted) It caused my birthfather and brother both to die due to them not knowing about this over 30 years ago. Also can anyone answer what the benefit is in knowing you have this. Are there certain other precautions I should know about?
Thanks for writing Dina. I think I may have answered some of these q’s in my reply to your other comment above. But let me know if you’d like more information than that. It really is worth getting a diagnosis. It can explain soooo much! (As you noted, you have this plus so much more.) To paraphrase Dr. Afrin who paraphrased Occam’s Razor: do you really think there are 57 different things wrong with your patient, or might there not be just one or two systemic explanations? NB I do strongly suspect you from your description. And I’ve yet to meet a fibro patient in real life who does not pass the Brighton Diagnostic Criteria (not the confusing closely named Beighton – with an “e” – 9 pt bendy scale only) for HEDS. You can score a zero (0) on the 9pt scale and STILL PASS the Brighton Diagnostic Criteria as I delineate here: http://ohtwist.com/about-eds/the-brighton-diagnostic-criteria/
You might enjoy my “Intro to EDS for Fibro patients” video here also: http://ohtwist.com/2014/09/03/intro-to-eds-for-fibro-patients/
Cheers.
Good gracious… I recently came to the realization that my oldest son has it, but after reading this I realize there’s a strong possibility that I have it as well! I have so so many of the items on this list. But honestly I am at a loss as to what to do about it for either of us. Our pediatrician suggested a geneticist but I don’t know what good that would’ve done, plus that geneticist is no longer practicing in our area
Sorry to hear that Jennifer. The geneticist is only good for getting EDS diagnosed – they don’t help with management or treatment usually, aside from initial guidance and suggestions. (Dr. Francomano in Baltimore being a rare and worthwhile exception.) You need a good PCP who “gets” it, and is willing to be in it with you and learn for the long haul. I do feel it’s worth getting diagnosed though still in case you need to see some specialists or apply for disability later. (Leading neurologist and Chiari specialist Dr. Henderson requires a geneticist’s diagnosis to even see you, he’s in such high demand.) That said, no, there’s no cure, but… there are lots of helpful therapies and strategies, including nutritional that can help. (I’m back out of my wheelchair because of mine.) Check out the recovery stories and solutions at the bottom of my Resources page here and triage your top 3 issues: http://ohtwist.com/eds-resources/
Maybe I missed it, but another symptom(s) which needs to be included is prolapse. I had both uterine tilting and prolapse, (until I had a hysterectomy) as well as rectal prolapse, made worse by the uterus leaning on the rectum.
As well, we seem to be “lumpy”, for lack of a better term. I’ve had three surgeries for benign cysts in my life, all just clogged ducts of one kind or another.
I only wish I’d been able to add up all my symptoms sooner in life, as I did spend many years with a misdiagnosis and doctors fluffing me off as being a “hysterical woman.”
Thanks for your posts, love them!
Thank you, no, you did not miss it – I did not have it in the list – good catch! I agree, prolapses and herniations of all kinds are also common “extra-articular” (non-joint-related) signs and experiences with EDS, bendy or not. Adding now!
And your comment about being lumpy also reminds me to add that we’re finding lipomas (fatty lumps, often quite painful) and lipedema (an adipose tissue disorder causing unavoidable weight gain especially in the lower half but notably stopping at the ankles) to be quite common.
Ironically, this is sort of starting to match my Common Comorbidities post, but that’s okay! People can arrive at the conclusion by multiple routes. Thanks for the input!
“Paradoxic reactions to medications, strong or strange reactions, need for increased novocaine or lidocaine” <— New doctors don't believe me. They always think I'm crazy because I don't try to hide that I have mild persistent anxiety and feelings of breathlessness… (even if someone's "crazy" it's screwed up to dismiss them). Anyway, they sure believe me when they give me something and I have a black box effing reaction.
I just got diagnosed with vocal cord dysfunction today. I want to phone all of the old doctors and tell them "my therapist disagreed with you about me having an 11-year panic attack that looked like asthma that triggered strange gasping. She was right." Of course I won't phone them, but I am annoyed. It seems like older doctors often have never even heard of hypermobility syndromes. I'm sticking with younger, modern trained doctors from now on.
Also, almost everything on your list applies to me. Good work!
Aw thanks, so glad I could help validate your painful experience, but sorry any of us have to go through so much invalidation from so many doctors. If they would just believe us, it would save so much time and money -and pain! I did end up emailing one past doctor who was nice but who under-diagnosed me with Chronic Fatigue Syndrome to let her know the “real” cause of all my fatigue. I knew that wasn’t quite right, but it took me another 20 years to find the real answers. I resisted flaming a few others. And have brought my mildly narcissistic and stubborn PCP “with” me, as he’s been a willing student since I figured things out.
Trust – and heal – your gut, always. But yes, it’s exhausting to not be believed, especially regarding anesthesia and pain meds. Stay strong, better luck!
I am wondering what your thoughts are about mcas and whether it actually can cause eds. Many of us have these onset storms, and some people also seem to recover some function when taking natural mast cell stabilizers (like high dose vitamin c and the Cusack protocol). Do you know of any examples of edsers being cured through conventional (by which I mean rx) mcas treatment — like with dr. Afrin?
That’s a really great question I don’t have an answer to yet, sorry. I’m up in the air about that theory – I can see both sides, frankly. I do think extra mediators from mast cell activation can mess with our extra-cellular matrix, thus messing with our connective tissue formation. But what I can’t square is why so many of my friends with much worse MCAD symptoms (any form, Masto or the new dx of MCAS coming out October 2016 in ICD-10) are so much stronger than I am in many cases – I.e, they shock sometimes daily, are much much sicker MCAD wise, but some are still working full time, and one even runs a farm. All walking just fine. Not formerly suddenly wheelchair bound and still struggling to keep walking like me now. Though yes, I know some who are too. I.e, it doesn’t correlate neatly in my observations -yet.
How come I am not much sicker MCAS-wise (though I experience plenty of low level trouble) but am so much more hypermobile/plastic/weaker? I didn’t notice a lot of anaphylaxis during my onset “storm” of 2012 either. I do recognize more signs in 20/20 hindsight, since I didn’t even know about MCAS at that time and had normalized low-level ana all my life like so many of us- I learned about it later in 2012 from Patricia Murray-Wood on Twitter when she followed me as @Mastocytosis and from @PrettyIll – Dr. Driscoll.
But, I do read of many people experiencing what you described – onset/increases in hypermobility commensurate with MCAD flares. So I don’t discount that either. Just hard to say – which is the chicken and which is the egg. And does Dr. Sharon Meglathery’s RCCX and illness theory explain it all, perhaps at least in those of us with the as yet poorly defined HEDS as outlined here?: http://www.rccxandillness.com
Mind you I love Dr. Afrin and think he’s a genius. (I’m dying to get a copy of his new book to read, “Never Bet Against Occam”, link below.) I really like his thinking – outside of the box, analytical, listens to his patients and connects more dots than most. (And works heroically hard to see and treat oodles of us when others won’t. Including many in the regional PNW MCAD support group I currently lead.) So I am not going to dismiss anything he says very quickly! I just take all I hear/see with a grain of salt, plus am weighing against my own (weird) experience. It’s a darn good Q! Afrin’s new book (just out April 2016):
http://www.amazon.com/Never-Bet-Against-Occam-Activation/dp/0997319615/ref=sr_1_1?ie=UTF8&qid=1460753656&sr=8-1&keywords=Lawrence+Afrin
Hi iv been diagnosed with Eds type3 an over past few months have been my worst ever I’m constantly tierd an in pain my bowels are terrible 1min diarrhea the nxt constipated. I’m fed up of going to my doctors as they just look at me like I’m a hypercondriac. I just want sum help from them with pain management an physio therapy but I’m getting no where even tho iv been diagnosed by genetics. I’m so depressed an feel so alone with this I wish I could find a doctor that understands what it’s like to live with Eds type 3 or any type of eds really. Lately my eye lids are drooping so servery that my eyes constantly look tierd iv been told to have bottox but my mam had that an it didn’t help so she had eye lift an now she needs another, my mam is in a wheelchair an only now getting the support she needs but iv been told mine is so bad that I need walking aids an I’m only 36 my mam wasn’t as bad as me at my age so I’m really scared of losing any more independence as I have no family help or doctors support I really don’t know where to turn any more I feel life is just to hard ?
Sorry I missed your comment before now Jessica Jones – I’m so sorry for your terrible experience. And an all too common one, I’m afraid, which is why I am writing – to help shed light on it and bring more doctors on board hopefully. But meanwhile, to empower you all, the patients.
Check out my resources page for some fo the best info to take to your doctors and also see the recovery stories near the bottom. I’m so glad my geneticist suggested Vit C and magnesium to me as helping when I asked in 2012 – they got me back out of my wheelchair and I’m *almost* ready to work again. (If you are allergic or sensitive to corn which is used to make cheap OTC Ascorbic Acid based Vit C supps, try to find another form like Sago Palm based C, or camu camu, or rose hips.) And we recommend other forms of mag also. (Some can only us mag “oil” – hydrochloride flake solution – on their skin, or epsom salt baths.) I’m now doing even better with the addition of the Cusack Protocol also listed here:
http://ohtwist.com/eds-resources/
That said, getting a handle on my MCAS reactions also greatly helped – that caused all my alternating diarrhea and constipation. (I’m so much more regular now, glory be!) I did best by going on the GAPS diet to both temporarily eliminate all but one food, and to help heal my gut (we all have signs of leaky gut, no surprpise also, lending to some of our trouble). It’s hard, but worth it, here: http://gapsdiet.com.
If you can’t handle that, at least do a food journal, and try at least eliminating gluten, and also dairy (which triggers the body/is cross-reactive to the body like gluten) if you can manage it. Yes, hard! But oh so worth it… at least for me. Trying to lower stress and avoid high histamine foods (leftovers, fish, ground meats, hard cheeses) should also help a bunch.
But every body is different, you have to find what works for yours. But there IS a little hope and help, kay? Also, look for a local support group here:
http://ohtwist.com/eds-resources/finding-support/
Hugs! Jan(droid)
I’ve been on this journey for about 5 yeats now. I had a triple hit in a years time (car wreck, blood clot in lung and nother wreck). After that I became extremely fatigued and unexplainable pain everywhere. I’ve tried to talk to my doctors about EDS and I’m always told I don’t fit any areas. I’ve been diagnosed with fibro, cfs, bipolar and migraines. I have so many of the above listed that I believe it is time to “educate” my doctor and possibly find a new one. Hopefully my neuro will be open-minded.
So glad I could help you connect the dots. Sadly, most doctors only know about the grossest signs of the rarest types as yet, and still think it’s really rare, so you will keep running into this resistance without better information at hand to show them. Be sure to troll my resources page for some of the best info. Castori et al in Italy cite as high as .5-2% show signs of the Hypermobile form of EDS back in 2012 – far from rare! (That’s 1 in 50.) I’ve seen a Cincinatti doctor show a study that found 1% in their area (1 in 100) – again, far from rare. This just isn’t widely known yet.
And who knows what the results of the recent International Symposium in NYC shared – they will be sharing this finally at the Learning Conference in July this year, so we have to wait until then. (I think they’re compiling all the findings now.) Trust – and heal – your gut, always. And good luck: http://ohtwist.com/eds-resources/
I went for years knowing that something was wrong with me. I went through a few general practitioners, many orthopedics, chiropractors and everyone said I was crazy, and I was young and healthy or would “bounce back”. You don’t “bounce back” from a fractured vertebra after hyper-extending your spine so bad you should have split in half. I finally started seeing a neurologist for numbness and I hit the jackpot with him. He not only figured out that I had EDS, he apologized to me for the lack of medical support I had received before him. He was the only doctor that actually listened to me, took copious notes, and was able to connect the dots to diagnose me. The sad part is that my orthopedic completely dismissed his diagnosis and said that my beginnings of arthritis in my knee and extra joint flexibility is “totally normal”. I’m 36…and to me that doesn’t feel normal at all.
The list you provided makes my diagnosis even more clear as I have more than I’d like to count, and made me realize that my oldest son is most likely also going to be affected (W sitting, Sensory Processing Disorder with high pain tolerance for starters), his younger brother maybe less so. It is very discouraging to be reminded of how narrow-minded some medical professionals can be. I feel so lucky to have met my neurologist and even though there is no “cure”, I at least know what’s finally going on and hope that others can find the same so-called relief as I did.
Gosh I’m so sorry for your terribly long painful journey to diagnosis also, but thank heavens your neuro finally figured it out! Why I’m blogging and writing – to try any way I can – desperately – to help many more patients AND doctors connect all such dots sooner. The ortho sadly thinks all your issues and early arthritis are “normal” precisely because it is so darn common and not rare at all!
We are their frequent medical flyers after all, so we are who they see all the time. And in the milder (subclinical) cases as I was pre-2012 and you were earlier, they think it’s no big deal because we are not disabled – yet. Sigh. I’m sorry for your son, but… thankfully you both have some answers now and know you’re not losing your minds, just your bodies – and there’s even some hope and help there.
But at the very least, you are no longer alone! Welcome to the giant “Clan Dumpty”, where no one can put us fully back together again – yet.
I believe this is comorbid with gender dysphoria. I know multiple (female to male) trans men with this and many (male to female) trans women seem to have hyper-mobility. Autism is also significantly elevated in the transgenser community.
Like you said above, what are the odds of having three, four, five, etc. rare conditions and dozens of symptoms from common conditions? It’s more likely there is an underlying systemic condition.
It will be interesting to see which chromosome is involved in EDS, autism, and gender dysphoria and if there is a common cluster of genes influencing these differences.
I’m having trouble getting a formal diagnosis, so far one doctor has diagnosed me and the primary care doctor he referred me to decided he’d rather holler at me and advocate against hormone therapy than practice medicine that day! Another issue is my arthritis has become so bad I can’t demonstrate that I’m “flexible enough,” though I remember being flexible up until my early twenties, when the ptosis and stiffness appeared almost over night. I’m very frustrated with the medical community. This is the third or forth condition my doctors have missed, which I figured out on my own.
It’s quite frightening to have this condition, and many other comorbid health complications, when so many doctors have tunnel vision about disease processes and cannot see the patient past their preconceived notions. Occam’s razor should have them asking deeper questions. Perhaps there isn’t time to think during these fifteen minute fly-by visits.
I can’t agree more, and have observed the same comorbidity in the LGBTQIA community along with a trans friend of mine who volunteers in the community. (It’s so hard for him to watch his fellow travelers suffering but so few are open to this information!) That said, Dr. Sharon Meglathery may have hit upon the gene cluster that may explain this all here:
http://www.rccxandillness.com
I introduce all the major overlapping comorbidities I’ve seen along with her hypothesis here:
http://ohtwist.com/2016/02/17/the-chronic-constellation/
I’m so sorry for your diagnostic struggle but, I assure you you’re not alone and I urge you to trust – and heal – your gut. There is some hope and help as I also describe here:
http://ohtwist.com/2015/12/03/trust-and-heal-your-gut/
I am back out of my wheelchair and walkling again – albeit with one Lofstrand crutch and a limp still, but… a far sight from where I landed 4 years ago (in early 2012) when I finally (finally! after 25 years of dismissal as “just depressed” because I was a woman) got diagnosed. BTW, I find lots of hope and help for our very real comorbid depressin – I’m increasingly convinced it’s mostly driven by allergies now as I describe here:
http://ohtwist.com/2016/01/28/depression-and-eds-and-mcad/
Meanwhile, try to find a local support group if you can. I have links for doing so here: http://ohtwist.com/eds-resources/finding-support/
Good luck and stay strong! We’ll eventually bring all these tunnel-visioned doctors around…
Wow, what a help your posts are. My 13 year old daughter received a diagnosis of EDS and possible POTs this week after months of injures, dislocations. We have struggled to get in front of the best dr to diagnose. Even staff at hospital were flummoxed as to who to refer to, thought it was in my daughters Head and she was deliberately injuring her self or I was an overprotective mum, we had an admission 2 weeks ago with severe inspiritory Stridor, again they think it’s in her head even though been struggling for 2 weeks now, asked for speech therapy to help as been told best way forward, Drs offered CAMHS! Thank goodness for an amazing geneticist who had reassured and diagnosed , now just need to find a supportive Paed dr to support my daughter through the journey we seem to have found ourselves on.
Interestingly my older daughter displays many of the Symptoms although not hyper mobile to the same degree and although I have been diagnosed with Anklosing Spondalthropothie many of my Symptoms fit EDS
You’re quite welcome, so glad the info is helpful! So sorry for (but not surprised) at your lengthy diagnostic journey. (Why I’m writing! To help shorten it for everyone else, hopefully.) Anyway, fellow patient Dr. Sharon Meglathery’s RCCX hypothesis may well explain why the variable presentation in your family as I introduce it here in this post. Do follow the linnk to her RCCX Theory, which while crunchy, is worthwhile to read. It really connects all the dots I’m finding:
http://ohtwist.com/2016/02/17/the-chronic-constellation/
Good job sticking to your guns and standing up for your daughter. Please know there is also hope and help for the recovery journey, especially via The Cusack protocol http://ouredsjourney.weebly.com
Could you elaborate at all on the tendency to blow electronics? This one seems kind of woo-y, but… I have just discovered I have HEDS and we’ve had a family joke for years that I’m a battery vampire since any watch I wear will die within a week and every laptop I use ends up with a useless battery that refuses to hold charge. Is there any actual plausible scientific mechanism for this? Because that would be kind of mind blowing if even my battery vampirism is connected to this web of insanity!
Lol – I love it, “battery vampire” – may I plagiarize that? My Reiki master would love it! There is only one electronic clock she has ever been able to keep running in her apartment because of this problem! And yes, I agree it’s a bit “woo-y”, but… it comes up ALL the time in the support groups, so no, we’re not alone at all. Alas, I don’t have any scientific data/studies to back us on this yet, but… I can tell you I personally blew 3 out of 4 of the engineering department computers while simply trying to replace memory sticks in them while working for the City of Milwaukie, OR in 2010, so trust me… it’s very real! (And yes, I knew how to ground myself – it didn’t help.) I told my boss to leave me back in the office pushing papers and electrons via my keyboard: I would do much less harm! (She gladly obliged.)
My personal theory/experience/observation is that all hypermobile people conduct (and hold) a charge much more readily for some reason – I have a feeling we tend to run acidic for various reasons I’m sure some one smarter than I could elucidate. (I bet Dr. Sharon Meglathery has a theory on this, see her project at http://www.rccxandillness.com – but only on a slow day with plenty of time, a snack and some water, it’s another deep site.) And here I’d been blaming my trait to “blow things” (and my curly hair) on playing with a Tesla coil while growing up all these years only to find I wasn’t so special after all… 😉 Welcome to the giant “Clan Dumpty” – of Humpty fame, right? We’re still trying to put ourselves back together again… while not blowing any more electronics in the process! Yes, you have found “your people” . 🙂
I have EDS. I have to wear shoes whenever I vacuum. If I vacuum in bare feet, I get electric shocks that come up through the floor into my feet. This happens with any vacuum, in any place that I’m in. I also get a lot of static electricity when I pet my cat. It bothers my cat, so I have to moisten my hands a little before petting. That’s it for me and weird electrical issues, for what it’s worth. :p
Ha! Defo don’t vacuum and THEN pet the cat, lol! yes! I think the air rushing through the vacuum builds static charge in us quickly.
I also don’t vacuum my computer (with shoes or not) ever for this reason… I use compressed air to blow the dust bunnies out and then suck them all up outside the pc.
Thanks for sharing!
Wow I’ve had this happen. Plus cell phone battery drains worse in my pocket. Watch batteries don’t die that quick with me but don’t last like they should. I wear a kinetic one now that winds by moving my wrist
You’ve found “your people”, lol! And I’ll have to look into that style of watch… I do also blow or drain normal digital ones.
Amazing. So helpful!!!
Thank you!
Thank you for your list. I have been discounted by many doctors because I don’t have stretchy skin. It took a aortic aneurysm for my cardiologist who pulled my skin and said hmmm maybe you have a less severe form to refer me to a geneticist. I have vascular eds.
You’re quite welcome. Glad it could help though very sorry to hear you turned out to have vascular EDS! 🙁 Best of luck to you.
This seems minor in comparison, but affects my life personally. Could trouble swallowing cause loud swallowing? I’ve been looking for data on this. I feel everything slide down my throat when I eat or drink and it’s really hard for me not to make noise when eating. If someone with misophonia is around when I’m consuming something I tend to get glares.
I honestly couldn’t say if it would make swallowing louder, but it seems plausible to me. Which would be very unfortunate if you live with someone with mysophonia who is very sensitive to such sounds yes. (An unfortunately combo.) Not sure what you can do about it except try to avoid eating near the sensitive people/person whenever possible? But yes, trouble swallowing is very common with EDS for several reasons, including weak laryngeal tissues, impinged brainstems and mild or more Chiari malformation, and cranial-cervical instability. Toss in comorbid MCAD of any kind, which can lend to swollen tissues and our deck is stacked, sorry. Better luck…
My 10 year old daughter was just diagnosed with EDS hypermobility type. (She also has Juvenile diabetes!). She was diagnosed by a pediatric rheumatologist due to her weird symptoms, including recurring fevers, that’s where we were referred to. So the rheumatologist had me schedule her for PT/OT to get her muscles strengthened up. We have that appt in about a month. So my question is will the PT be the dr we see re: her EDS or what kind of doctor does one typically see for this?? I know it is not a rheumatologist. Thank you!!
THe PT is just one member of a “team” you will ultimately end up assembling to deal with all her issues as they arise, when they arise. Make sure the PT understands she is HYPERMOBILE, meaning “very plastic” (in their terms), so they don’t accidentally injure her. We can and do benefit from PT but only when done correctly for hypermobility/our bodies.
You should have a good primary care internist who will manage all her care, and make referrals out to the specialists as needed, just as you did to see the rheumy who diagnosed her. BTW, I highly recommend a naturopath and or a nutritionist to work on diet too. (I got better after fixing my diet and increasing vit C and magnesium the most. Find forms you tolerate tho – key.) Even better, a functional medicine doctor would be ideal if you can find/afford one. (That’s an MD with sort of ND training added on so to speak.) You will just slowly grow the “team” as issues arise and she needs to have them addressed – but not before. I would get a baseline echocardiogram done, but if she’s fine, then don’t worry for another five years or so after that unless they tell you otherwise.
But ultimately sadly we patients (and parents) end up being the “project manager” for it all. Yes, it’s a lot. But you are on the right track. Congrats on getting her diagnosed – that’s a huge step and success! She can/will get a bit better in time. Patience and perseverance is key. (This is where our stubborn streak can be useful.) And, kknow that hormonal swings can wreak havoc with us – progesterone makes you more lax, and both it and estrogen are mast cell triggers. And MCAD of all kinds is commonly comorbid. More on that here:
http://ohtwist.com/what-is-mcad/when-to-suspect-mcad/
HTH, good luck. Stay strong! You’ve got this, and you’re not alone! x
Also see this site for great PT info for EDS patients: http://www.muldowneypt.com/ehlers-danlos-syndrome-information/
Thank you so much!!!!
I have 56 of the symptoms. I have mast cell activation syndrome, interstitial cystitis, pelvic floor dysfunction, SIBO (I think) I’m taking an antibiotic for it to see if it helps because testing me must be too hard for my doctor. Ehlers Danlos, ‘fibromyalgia’ chronic fatigue syndrome, apneas, chiari 1, empty sella, POTS, degenerative disc disease, etc. I didn’t know Sibo was related but makes sense. Thank you for these lists and the update about EDS classifications in March 2017. Its people like you that helped me find out my issues not doctors. Keep up the great work!
You’re quite welcome, glad the info is helping, though sorry you also suffer from so much of it. I like to say we put the “syn” in “syndrome”, heh. Also, fwiw, I found oregano oil to help my SIBO, in case you either don’t want to to an antibiotic, or it backfires on you (you react). I would avoid Cipro and the other fluoroquinolones in all cases as I write here at least:
http://ohtwist.com/2014/04/24/avoid-cipro/
And consider working with a naturopath or functional medicine doctor (MD) to restore your gut health (possibly upping your stomach acid if needed using betaine) to help prevent recurrence of the SIBO. Good luck!
Sorry for the double post but I just read more of the comments and I too am on the Deborah Cusack protocol (polysaccharide protocol) I started it two years ago before I even knew for sure I had EDS but knew I had Chiari and I had a hunch. It has been a God sent. It hasn’t ‘cured’ me but it makes life more bearable. I haven’t given up over the last 2 and a half years to find solutions to our problems. I figured the more I dig the better shot I have of not living like this forever and helping my kids and others possibly. I remember others thought I was crazy for taking the protocol but I’m so glad I did. It also helps intristitial cycitist a whole lot which I didn’t know until I ran out of distilled aloe. I recommend the protocol for those suffering! Also because of my IC I cannot take vitamin C otc vitamins without having a huge flare. Is there anything else you could recommend that may not harm the bladder lining that is damanged from my mast cell activation syndrome most likely? Thanks!
So glad to hear the Cusack Protocol is helping you too! I found the PQQ to really help me most: I stopped peeing like a racehorse all the time finally ahh…! If you react to cheap OTC Vitamin C from ascorbic acid, that means you react to corn, and thus any thing made with corn starch fillers too. (Ascorbic acid is made from corn.) You might try other forms of C (carefully, only one at a time, wait at least a week or two an dpreferably a month to see if notice a difference):
Sago Palm based C
camu camu
rose hips
tart cherry juice
Moringa Leaf (see Moringa Tree of Life)
brussels sprouts and spinach (beware salycilate and oxalate issues with greens)
And indeed, be careful not to start developing kidney stones as I think I’m just barely beginning to do from too much C plus calcium and oxalates. (I’ve been hitting the kale juice a little too hard lately, oops. Cutting back and adding lemon to my water now to hopefully dissolve those puppies.)
The PQQ may also help your bladder lining if not on it already. (Pyrroloquinoline quinone I think it is.) And keep the water going in with electrolyets (but not sugar) to help it “stick”. HTH good luck! Someone also just shared this with me on FB tonight: http://physicianstowomen.info/interstitial-cystitis/
Cheers – Jan
Thanks for this information. I have been diagnosed with HEDS. I absolutely LOVE greens of all kinds, and now have lots of beautiful spinach in my garden. I have noticed that every time I eat a lot of them, I get swollen and sore lymph nodes. Could this be MCAD from the oxalates? I have suspected MCAD anyway, due to some skin issues and opposite reactions to certain things. I am the only person I know that sets on fire with an olive oil bath! Anyway, I found that taking C Salts seems to help me a bit. Have you tried that at all? Take care fellow zebras!
Hi Susan, yes, reactions to oxalates are pretty common in our community, I don’t know why. So that result doesn’t surprise me, sorry. But don’t stop eating your lovely spinach altogether – just space it out a lot more or mix it in with other things or cook it down. And now you’re the second person to react to oil. 😉
I’m not sure what C salts are – is that cell salts? Like these?
https://healthygoods.com/blog/what-are-cell-salts/
And no, in any case, I haven’t yet. Do you recommend some? Cheers, Jan.
Omg thanks for this. Trying to figure out what’s up with baby. She is not failure to thrive so GI, neurology are apathetic. How about childhood migraine variants? baby has BPT, super rare. There are other kids with EDs and bpt that much I know. Astigmatism? Food protein induced entercolitis to most protein? She Is developing normally for now thank god, but…. epicanthal folds? Single palmar crease? We both have it. No she doesn’t have any obvious disorder, is developing months ahead. Reflux? Microarray, metabolic panel are running. Geneticist said heds genes are not known. I assume it’s a collagen or elastin issue of some sort which is how I even stumbled on eds – was unaware befow
You’re welcome and yes, I might suspect some possible form of connective tissue in her from the things you’ve described, but it is almost impossible to diagnose it in babies unless they show signs of a rare form and get molecular testing done and something matches. You may just be stuck suspecting for a while until she’s old enough for doctors to differentiate infantile flexibility from any “extra” hypermobility she may have if any. But yes, this is all sort of a package. Why some are more/so afflicted out of the womb I’ll never know, but you’re not alone. Look for the Masto Moms group on Facebook. Or check out http://tmsforacure.org for some help with the reflux/GERD.
And trust your gut – your mother’s instincts are virtually always right. Just think marathon, not sprint, okay? And avoid any dyes, chemicals, fillers, GMO’s etc. (And chlorine and fluoride.) Also mind what you’re eating (and how you’re feeling – are you stressed out? Highly anxious? Or calm?), and notice any effects on her if nursing. And consider balancing her gut biome with the help of a functional medicine doctor or naturopath later as this mom did for her autistic son (you don’t have to use exact same method – some can succeed with regular oral supplementation once the child is old enough to handle such a thing) http://www.healourlittleones.com/?p=837
In all cases, try to work with her doctors patiently, but persistently and do not panic. You will “thread the needle” of her health issues in time, I promise. Despite some common themes, it’s ultimately as individual as fingerprints for all of us. You sound like a great determined mom. I’m sure you’ll figure this out sooner than later.
Good luck! Jan
WOW! What an incredible resource to have this information gathered in one place.
I have struggled with pain my entire life, hypermobile joints as a youngster, but stiff / tight joints and muscles fascia as I get older.
I have a long list of the other symptoms / comorbidities you mentioned above, as to many members of my family. I am the first of my living relatives to suspect and pursue a diagnosis of connective tissue disorder. I recently found out that my maternal grandmother had a brother diagnosed with osteogenisis imperfecta and died before the age of three. This motivated me even more to seek clarity for my family and myself so we can be informed and empowered to care for our bodies and minds.
I feel like I’ve lived my life in this silent suffering, telling myself it was normal (normal for me!) body sensations, all the while feeling exhausted and more desperate as I aged and pain and medical complications arise and worsen. I am 32 years old determined to obtain the most wellness and best quality of life that I can.
I’d dare to say that one of the biggest triggers and stressors for an EDS (CTD) patient faces is the indifference and denial from medical care providers, it is for me at least.
A couple things stand out to me: I’ve been thinking a lot about hormones and relation to my ‘flare ups’ or we could call them ‘cascades’ I have learned 🙂
I noted a significant decrease in symptoms and overall wellness after the birth of my twin boys and taking dried placenta pills (my own placenta encapsulated after it was dried, no herbs or anything else added). I felt so incredible that I actually ‘craved’ more placenta pills once I ran out. Have you heard anything similar to this? I am interested in doing more research in this topic.
Also, I’ve been noticing an increase of lights ‘going out’ when I pass by them, this is something I have noticed most of my life, and it seems to increase in frequency at times. Do you have any more information or would you be willing to have more conversation regarding this? I’ve always found it a striking phenomenon and have never found anything to really begin explaining it. I find it fascinating that you listed it as something that EDS patients report!
Yours in the Journey,
Shelby
Thanks for the kind words, Shelby, I’m so glad my post is helping you to confirm your suspicions and pursue this further. (Trust – and heal -your gut always, I say!) Our diagnostic journeys are very parallel minus the child bearing – I never hatched any. But I also had many odd issues and symptoms and troubles that always got written off as “just depression” or anxiety until I fell apart suddenly and hard in my mid 40’s from what I now believe to be hormone driven onset “cascade” from peri-menopause in me along with some cumulative stress.
I say this, as my elderly aunty Sr. Kathleen (slowly declining in the Holy Child center back east) also sort of “fell apart” in her 40’s, despite living a sedate life as a Catholic nun. So while stress may have played an additional role for me, we’re definitely related – we both have bum right legs now that give out easily (are loose) with wonky loosely fitting foot bones (my arches are trying to fall but not succeeding – yet).
I think your instincts about hormones driving our flares are bang on – Dr. Tinkle stated the progesterone makes us more lax in his original book on Hypermobility Syndrome (whence more women getting diagnosed even though the EDS technically run equally in both dominant genders). And both it and estrogen are mast cell triggers for our lose as well, also contributing. (Some with MCAD find their joint laxity increases with their MCAD reactions.) To whit:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3377947/
Be sure to rule out OI fully with your family history of course. I now think many of us can/may be “carriers” of some more rare types and other CTDs like OI and just not know it, and appear to have hEDS or an HSD (new dx since March 2017).
And, you might like what else I wrote/observed here that may further confirm your suspicions. It’s totally unverified/unfounded yet, but I am eager for science to catch up and prove or disprove these observations I’m having of thousands:
http://ohtwist.com/2016/02/17/the-chronic-constellation/
And… yes, we definitely blow electronics lol! Just ask my old boss – who sent me to replace memory sticks in the engineering department of the small city we worked for one day. I figured the first one was a fluke. The second one, I started to get nervous. After number three, I told her to leave me back in the office filing as much as she wanted, lol! I wasn’t “safe” around the pc’s, and wanted to “first do no harm”. (My poor colleague had to “clean up” after me and repair or replace all those machines I was just trying to upgrade with memory, heh.)
Anyway, it’s true. Here are some more things we find “common” in our families, but not necessarily in the general population you might enjoy too:
http://ohtwist.com/2016/12/02/what-is-normal/
Thanks again for writing. Best of luck in your diagnostic journey – definitely trust your gut. Hugs,
Jan
I was recently diagnosed with Blepharitis and have previously been diagnosed with EDS3(hypermobility type). I’d really like any link to info relating Blepharitis to EDS / hypermobility syndromes. I can’t seem to find it mentioned oin the new criteria for diagnosis. Any help appreciated 🙂
That’s because there is no official link, nor mention of any outside of my blog that I’m aware of yet. I’ve just observed it to be comorbid. I suffer from an intractable case myself.
My hunch is that it’s due to the commonly comorbid primary immunodeficiencies I find come with the condition so much as I describe here. It leaves all of our environmental interfaces “weak” and unable to fight off infections very well, ironically, despite our often over-active mast cells as well:
http://ohtwist.com/2016/02/17/the-chronic-constellation/
NB The above is all pure hypothesis on my part. I look forward to medicine uncover more of the real drivers if different than the above. Meanwhile, yes, blepharitis is a bugger! Sorry you share it.
I am a four on the Beighton Scale, but they are all the passive wrist/finger ones. I can’t hyperflex my elbows or knees. Years ago I could touch both palms to the floor, but no longer. I’ve been told by numerous physical therapists that my chronic back and neck pain are because I have a hypermobile neck with muscles too weak to hold my head up (and carry the strain instead in my neck). I have 26 of those related symptoms, but not the really obvious flexibility ones. I was always clumsy, not athletic. I see my rheumatologist next week, and I’m trying to figure out if I should mention the Beighton Scale score of four, or if since it doesn’t fit the new 6+ (even historically I am not sure if I’ve ever been more than a 5 – but not sure I ever tested enough when younger either.) Do you think it’s even worth mentioning, or is it really just unlikely that someone who can only do the weird flexibility stuff in her hands and neck can’t have a hypermobility disorder?
So you would be a prime candidate for a diagnosis of the new category called Hypermobility Spectrum Disorders they just recognized and introduced last March 2017 for those who have many signs of a systemic connective tissue disorder, but are negative for the grosser signs of the more rare forms (including Marfan, Sticklers and OI and all the EDS). You could then be considered for one of these now:
http://ohtwist.com/hypermobility-spectrum-disorders/
I.e, the main difference is you just aren’t bendy enough, now, or ever in the right place (key) to pass their beloved 9 pt Beighton scale, but… you are clearly suffering from SOMEthing that affects your connective tissue just the same.
I like to say dogs don’t bark for no reason ever (even if their reason doesn’t make sense to us), and our bodies don’t “bark” (hurt/injure/tear/sprain/strain, herniate, etc.) for no reason either. Just because we don’t have all the answers about the cause doesn’t mean you’re not suffering and couldn’t and shouldn’t still be treated pro-actively with proper management and support. We just don’t have an easy genetic marker to hang it on, if we ever will.
BTW, EDS or not, do yourself and your doctors a favor and download all 18 of these papers describing the entire new EDS/HSD nosology and diagnostic criteria now while they are still free here. (Don’t print them all – it’s over 1″ of paper! Just the most pertinent ones for you. Also, do this on a PC/laptop, too many/too big for a phone.) The Ehlers-Danlos Society originally said they would only be free for 3 months, and I’d hate to see the opp to get them go away for you. Even if you don’t think you need them. But this includes the new HSD I just described above as well okay? And share with your doctors!
http://onlinelibrary.wiley.com/doi/10.1002/ajmg.c.v175.1/issuetoc
Sigh. Thanks for your support. I saw the rheumatologist yesterday. He agreed I had “some hypermobility,” but because it wasn’t in the elbows or knees, he dismissed it. He said it doesn’t affect diagnoses if it’s only in my feet, wrists and neck. He tried to dismiss me with a fibro diagnosis and a generic packet of info on treating fibro. It was frustrating, to say the least. At the same time, I was feeling very dizzy and my blood pressure was reading incredibly low. Any chance the very low blood pressure is a clue? I’ve been low all my life, but yesterday was into “scary low” territory. Really confusing to me that that was just dismissed as no big deal…
For what it’s worth, I also just ignored your advice and tried W sitting. I can do that :-p I can also do the reverse Namaskar. I can’t tell if I’m extended enough to have true flying hand or not, but add at least two to my score on your unofficial list of additional symptoms above!
You mention blowing nearby electronics. Does anyone else burn out light bulbs when turning them on and off? I am forbidden in my house from most light switches, cause they seem to burn out quite often when I touch them.
I don’t personally – yet 😉 But I bet some others do! Some personal unofficial protips to help with this problem:
a) (try to) pick up your feet more, avoid “scuffing” which builds up static electricity, especially on carpets in the dry winter (I know not all can)
b) (try to) grab a metal door knob or railing or something that’s bigger and “grounded” to “discharge” any built up charge you are carrying
c) avoid petting the cat or dog before touching the light switch
d) don’t play with Tesla coils while growing up (smile)
Good luck!
Hi, a really interesting blog. I have just been diagnosed; before I was given a vague ‘we don”t want to label you, its kinda like fibro/ME non-diagnosis.)
Looking back, I had some symptoms in childhood/youth, particularly a lot of weird ankle injuries, bad scarring and early onset varicose veins.
What I was really interested in is that you mentioned a ‘cascade’ or ‘storm’ as you hit your 40’s. Could you clarify? I was 39 and considered myself pretty healthy at the time and then bam! overnight I had reflux so had I thought it was a heart attack, I had horrific body pain that would move around, dizziness and eventually even optic neuritis. This acute phase vanished in 6 months but I was never the same again…
Well, onset “cascades” or storms are going to be different for all of us. But yes, I would first suspect you of some kind of connective tissue disorder based on your brief description. And then, noting that it seems to be hormonally driven, likely progesterone if I had to guess, your “flare” sounds like a similar onset “cascade” or storm too.
NB that progesterone (and estrogen) are both mast cell triggers for our lose, and… histamine causes the stomach to produce acid, which would be common with our comorbid and equally unrecognized MCAD. Combined with weak hiatal sphincters and boom: your horrible reflux. (I thought I was having a heart attack once too – ask my friend Amanda about that!) Some back up info:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3377947/
https://bsd.biomedcentral.com/articles/10.1186/s13293-016-0113-7
http://journal.frontiersin.org/article/10.3389/fimmu.2016.00140/full
(Sorry, I double posted just oen link before. And not the other ones I also wanted!)
It’s my personal, very unscientific observation that people can experience “peri-menopause” meaning wide fluctations in the female hormone panels anytime after age 30 frankly. (My aunty and I both fell apart in our 40’s, but I’ve seen people go down any time after 30.) Why, who knows. But… it sounds like you rebounded a bit which is good. FWIW, many complain of greatly increased pain and joint laxity with PMS.
More on MCAD, a common hEDS comorbidity at last IMHO:
http://ohtwist.com/what-is-mcad/
http://ohtwist.com/what-is-mcad/when-to-suspect-mcad/
http://ohtwist.com/what-is-mcad/mcad-resources/
HTH cheers – Jan
Oops – except I’ll add that I DO blow the new “CFC” bulbs really easily and often. They are a huge expense for me. No cost savings at all – they never last around me, sigh. Not so much the old Edison style bulbs with filaments which I prefer for other reasons. Unsure about new LCD style, which I dislike (too bright/white for me).
I have had EDS all my life and known about it because my biological father and his mother were both diagnosed with it. So when I started bruising at age 4 my mother took me to my grandmother’s dermatologist to which I was also diagnosed with it. If I hit my elbows just right they not only bruise but swell to the size of golf balls. My knees get cysts and in college one dislocated. It has since done so a second time. I also had my thyroid removed due to being hypo and hyper active. Not sure if this is related. When I was pregnant I learned it made me high risk because the tissue in uterus might not be able to hold the weight and my daughter was 2 weeks early even though I had not dropped yet. If you develop a heart issue during regnancy they won’t let you push because you could rupture the aorta. Not sure if I spelled that correctly. I’ve had stitches many times including last summer when I scraped myself on my the edge of my dishwasher. The doctor said it Was like fileting my skin like you do a fish. It has not been a pain free life but I’ve learned to live with it and choose not to let it get in my way.
I’m so glad you got diagnosed so young! That is truly rare, though ever so slowly increasing thanks to the internet helping to spread awareness. I’m impressed with how you’ve just gotten on with life despite your challenges. I had not heard that about not pushing during pregnancy lest you rupture the aorta. I’m betting that mainly applies to the vascular type, or to anyone with an enlarge aortic root. (You did spell it correctly.) Good to know and makes sense. I’m just now getting back on with my life after five years of “rebuilding” myself after I fell apart so suddenly and so badly unexpectedly in 2012. I’m really glad, I wasn’t sure I would ever work (or walk) again. But never say never! Rock on, and thanks for writing, Jan
Omg I have 47 of these!! I’m just shy of 40 years old. I would also like to add that I have trouble “holding” chiropractic adjustments and I have a severe cervical disc herniation without history of an accident. Oh, and I blow light bulbs in lamps when flipping the switch on, and I cause electronics to malfunction; software “hangs” and apps crash, or my DVR player won’t load my saved shows, etc. Even my iPhone does funky things. Same with my truck stereo, connected to my iPod. :O
Thank you so much for this list!! (Applause)
Lol – you’re quite welcome! And welcome to the giant, and ever growing “Clan Dumpty” as I call it, of Humpty fame right? Where they can’t easily put us back together again, no matter how many king’s men come! (And they’re on zebras, not horses too.) You’ve found “your people”! (Or I have, anyway!) 😉 Cheers – Jan
I thought it was Dr Francomano who quoted, “If you can’t connect the issues, think connective tissues.”
This is an extensive, well put-together read. Thank you! I was searching to see if my Baker’s cyst was part of my EDS or if I should further pursue Lyme diagnosis. I am almost relieved to see it in the list, although I do have some unexplained ongoing systemic inflammation that I am not sure is related.
I’m sure Dr. Francomano has probably also referred to and/or quoted Dr. Heidi Collins, who co-opted that awesome phrase as the title of her talk. We’re still trying to run down the original originator of it, to give proper credit. So whover that is, hat’s off to you! In any case, yaeh, if our issues aren’t due to outright EDS, they could also be due to any of the myriad comorbidities we seem to also enjoy as I described here:
http://ohtwist.com/2016/02/17/the-chronic-constellation/
Cheers
I was a young woman who has been living with Epilepsy for 8 years. When I graduated one year later from high school I had bad migraines which became seizures, which followed by uncontrolled seizures up to 7 a day and as years went on my life stop. I lost my first great paying job and was not allowed to continue college because of my seizures in class. As a result my license was revoke. And it got to the point where I stop living I was trapped in the house because various times I was robbed and treated badly. In 2005 I decided to have brain surgery cause the seizures increased, and my life started to changed although the surgery was great it reduced my seizures but did not take them away and I was able to return to school, and I graduated with honors, and I do what I love to do sing, and write. In 2013 i heard about Doctor Lawson from my sister for his miraculous herbal medicine, I was curious to know how it works. I contact him and then I made an order of his product, i used his herbal product for mouths, His medicine has change my health and worked perfectly well and i am cure from seizure completely, seizure free contact this http://seizurestory.blogspot.com/2008/10/seizure-free.html to no more about Dr.Lawson
Glad to hear you both found something that worked for you! I approved this post a little reluctantly though… only because it appears you are trying to sell something. But… I’ll allow it only because I also know that I’m now better due to many “off-label” and holistic remedies and nutritional supplements myself, although I never had seizures. (Only myoclonus.) So I’ll simply add a cautionary note to all others reading: please take all such suggestions/advice with a grain of salt, always, and consult your doctors. But… in the end, we are in charge of our own bodies, or should be. If this turns into a marketing scheme however, I will remove teh comment, that’s all. (Note to any/all others wanting to target my audience to “sell” something, this is not a blanket permission to do so. I screen every single post/comment.) TY and best wishes to all.
I have 36 of these out of all you listed. I also have POTS,IBS,suspected chiari and EDS,thinking maybe an allergy conponent aswell and issues with recurrent UTI’s no matter what i do. currently waiting on a geneticist appointment and can do 8/9 on the beighton scale too >..<
Sorry – but not entirely surprised – to hear this Sophie. Best of luck pursuing support and diagnoses! x
Hello Jandroid,
I am 38 from the Netherlands. A few weeks ago I discovered that my face & neck skin stretches more than others. I never noticed and now I don’t even know if I had it before.. First I thought I was just aging. I felt the skin of my mother in law she is in her fifties and it was much more firm but I guess that is so different in every person. But when I checked te internet I saw a few youtubes and a blog https://mastcellblog.wordpress.com/journey/edsphotos/ . And then I thought well, I have the aged hands to, Peizogenic papules (didnt know that was not normal), and the way she can stretch I can too..
I found your blog and I saw the list en what I have is I bruise easily (but not as much as other pictures I have seen from EDS), Bruxism, Receding gums, Raynoud, Varicose veins (since my early twenties), when I was a child I inversed my upper eyelid for fun, since a few years I have the cracking and popping joints and left jaw since a year, I have lipedema since the age of 14, reverse namaste sign I can do , but I am surely NOT hypemobile, I have very poor temperature control I cant have heat or cold, velvet soft skin, breat ptosis, low blood pressure.
And I was diagnoses PCOS when I was 23. From then I went to holistic naturopaths, hospital told me to go on with the Diane pill, I didnt, I went to a naturopath en within a year it was gone.. from then I did a lot of research on good nutrition..so since the I eat a better diet the the most en since my 30 I do the Weston Price like diet which I take vitamin A en D en things like bone broth…
But as you can see, I have nothing with the pains or anything..and I feel almost quilty putting it here because many have such an serieus condition..
But I am a bit confused that I found this and all I have is within EDS but I dont have the more serious problems people with EDS suffer, although I think the very poor blood circulation is not good in the long term and can give me more serious problems getting older.
What do you think?
Hi Deb and welcome! I’m glad you found my blog. As I’m not a doctor, I obviously can’t diagnose (and you’re not asking me to), but from your description, I would definitely suspect you of having at least a form of the newly recognized Hypermobility Spectrum Disorders they JUST introduced last March 2017 as I wrote here:
http://ohtwist.com/hypermobility-spectrum-disorders/
If not actually a form of EDS itself. Because you say you are not really hypermobile though, that is why I would lean toward a form of the new HSD – it allows you to not be “bendy” – much, or at all. I *used to be* very bendy as a child, but am now very stiff and just “breaky” as a middle aged cis-gendered heteronormative female at 51. I’m not bendy almost at all any more except in my fingers and hands, but my joints sort of just come apart at the seams.
As for not feeling much pain or trouble from it – that’s also still possible, as some people are “hypo-sensitive”, meaning less sensitive than others to pain. And some of us (like me) are hyper-sensitive, meaning extra-sensitive.
The other trouble you describe are very typical of comorbid dysautonomia and possibly mild MCAS. Please explore the rest of my site when you can to learn more about those issues here and here:
http://ohtwist.com/what-is-mcad/when-to-suspect-mcad/
http://ohtwist.com/2017/01/17/wherefor-art-thou-dysautonomia/
Whatever the reason for our connective tissue variance and trouble, it lends to all of these systemic body-wide issues, and everything you described for as yet unknown reasons. I do strongly suspect you of at least a form of HSD now as mentioned, if not actual hEDS itself. Don’t underestimate your “talent”, (e.g. reverse namaste sign, etc.) mind. And I would talk to a preferred doctor and share that you *suspect* you may have a form of the newly recognized hypermobility spectrum disorders, if not an outright EDS itself.
And, lastly, not all people with true forms of EDS are severe – and some with HSD are quite severe. They just don’t meet the newly tightened and very strict new hEDS criteria the doctors are seeking for research purposes shown here:
https://ehlers-danlos.com/wp-content/uploads/hEDSvHSD.pdf
I.e, It’s not either / or so to speak. I.e, you can be mild or severe with either condition (HSD or EDS). Yes, this is hard to get our brains around. The doctors who classify these things are just super keen to keep the forms of EDS as “rare” for reasons I don’t understand.
And I’ll say this much: I don’t think they newly recognized Hypermobility Spectrum Disorders (HSD) are rare. But we have no data to go on yet as it was just newly “invented”. (I feel like Pluto, when it was demoted to a dwarf planet in 2006 remember? It didn’t change a spot…)
I hope that helps a little. Anyway, thanks for inquiring. And I hope you can start to get some answers with your doctors over there. Good luck and Happy New Year!
Hello friends: I am writing from Spain using the Google translator.
Sorry for the linguistic mistakes. From what I know of Eds, Similar situation is lived in Spanish-speaking countries, including Spain: Where it is so difficult to find a good doctor specialized and interested in treating us.
Over time I have collected information that can be useful for many zebra companions. I wish you could use these links if you wish, I would also like to draw on the information you have published. Thanks in advance.
A Spanish zebra with lipedema.
Gracias Thu! I have another Spanish friend with EDS on Twitter who volunteers for ANSED named Margo. I would love to see the links you have to share, yes. I welcome them in Spanish too – EDS does not discriminate as you know! (Neither does lipedema.) I think it is hard to find good doctors almost anywhere still. Thank you for reaching out to us here. And yes, you are welcome to share my information – just be sure to give proper credit is all, thanks. (The links in my resources are all publicly available information – no need to credit me for that. Just my original posts and writing like this page, thanks.)
Hello and thank you so much for this information & thank you so much for taking the time to offer your guidance. In many ways, my hEDS has always been strike at my body with a vengeance. I am now 43 years old, and was officially diagnosed 6 years ago.
It’s very interesting to me that there is a probable link between a “cascade” or flare and times of great stress, grief, or any other life changing event or trauma. That has been a pattern for as long as I can remember. My most intense flare began 6 years ago. It began suddenly, and just kept escalating for the next several years.
I can still remember that day in April, 2011. I was standing at a friend’s desk at work, chatting, and the next thing I know I began to feel hot, dizzy, and had intense ear ringing, with everyone’s voice getting farther away. The next thing I knew, 8 minutes had passed and I was more concerned about the looks on my colleagues’ faces. They were all terrified because they couldn’t even get a pulse, even with the most sophisticated equipment. Now, that wasn’t the first time I’d had syncope or fainted, but it was the beginning of what I know now was the fight of my life!
In the 6 months prior to that syncope episode, I’d been dealing with one issue after the next. Oral surgery to remove wisdom teeth (NIGHTMARE, as the local anesthetic did nothing to fill my pain . I healed so poorly and I had to have 3 more surgeries to get it right. Less than 6 weeks later, I began to just feel miserable. My stomach hurt so badly, a strange type of pain that I’d never known before. It felt as if I’d done 1000 sit-ups the day before. I saw my doctor, then a GI doctor, 2 visits to the ER, yet 2 weeks later I only got worse. No one believed me. Until one day, my appendix RUPTURED & almost killed me! 8 weeks after that surgery, I had to have another to reset and position my patella. The day in April that I referenced above was less than 4 weeks after the last surgery. I’ve always wondered if they were related to my “decline.”
Within 5 months, I was inpatient at Mayo Clinic for 3 months with organs failing. In a way, I wonder if I was fortunate to have my symptoms be so severe- doctors couldn’t just patronize me.
Oh, & I have every symptom on your list, with the exception of 3. I find it FASCINATING that IgA Deficiency is on the list! I received this diagnosis while inpatient at Mayo… I don’t know anyone else who has it, but what a shock to see a connection!! Again, thank you so much!
Ah bless you, what a severe onset cascade you had too yes, I’m so sorry! But yes, I also feel a little lucky for the same reason: they couldn’t just keep dismissing me as “just depressed”, heh. So far off the mark…but it shouldn’t take such severe cascades and onset storms to be believed. I’m inclined to start calling this “Gaslighter’s syndrome”, as we’re medically gaslighted until we become severe enough to be believed. (I feel a blog post coming on.) Google gaslighting if not familiar. (Basically, invalidation.)
Anyway, so glad you survived, and held on, and got some answers. We’re not losing our minds, just our bodies, right?
And yes, I can’t believe how much seems to come with this. I strongly suspect the RCCX Hypothesis may well explain this which I introduce in this post:
http://ohtwist.com/the-chronic-constellation/
It’s here, if you just want to skip to the meat and potatoes:
http://www.rccxandillness.com
Cheers – Jan “Dumpty” (of “Humpty” fame, right? smile)
My daughter (14 Yrs old) has cavus foot and we are searching for the reason. Neurology ruled out the a neurological issues and her muscle are good. So we are moving on.
Recently my sister was “semi-diagnosed” with eds. (Her doctor needs to do more tests). My sister doesn’t have cavus foot so my initial perusal of eds didn’t fit but my daughter can bend her thumb back and she can bend her elbows back slightly.
Does anyone have cavus foot as a result of eds? I did see some blogs that said it is possible. I just want to be able to be informed as we determine the cause. My daughter will need some kind of surgery so I am anxious. Fixing the foot might be the end of her issues.
Sorry for delayed reply – I was having a “Bed Attachment Day” today. (Reacting to yesterday’s food & drink and activity.) Anyway, I could swear on a bar of dark chocolate I have seen high arches (cavus foot) tied to either EDS or “just” HMS in one of the first books I got. (It’s much more highly assocaited with pes planus, or “flat foot” from fallen arches.)
So I just snagged my copy of Hypermobility, Fibromyalgia and Chronic Pain 2010 by Hakim, Keer and Grahame which I correctly remembered addressing foot problems, but couldn’t find that listed in a quick glance. Nor could I find a mention of it in Dr. Tinkle’s Joint Hypermobility Handbook either. But I *know* I’ve read it somewhere, because a friend of mine was admiring my feet one day, noting how “normal” they looked (thanks!) while sitting barefoot. (I’m super lucky to have decent arches yet.) And he proceeded to show me his, which had super high arches, tall enough to drive a Matchbox car through if you really wanted. I would never have noticed if he hadn’t said anything, but I immediately remembered having read that high arches were present in some hypermobile patients and told him so. (He has others signs IMHO, but being male they are very subtle.) You can see more recommended books here:
http://ohtwist.com/eds-resources/recommended-books
Anyway, short answers is yes, but long answers is darned if I can remember where I read this, sorry! That said, a quick google shows it to be more closely associated with another CTD called “Charcot-Marie-Tooth Disease”, which shares a lot of overlapping signs and symptoms with the forms of EDS and HSDs as shown here:
https://www.acfas.org/footankleinfo/cavus-foot.htm
I’m now going to keep trying to find my original source, because my brain is like a terrier, and will work at this until it’s solved. And… I did see in both books above that surgery is generally not recommended in hypermobile patients but… every case is different. Your daughter’s issues may outweigh the risks. (We heal poorly, and usually another nearby tendon, or ligament etc. will experience more or new strain due to whatever “fix” we did with the surgery.)
I’m sorry to have no easy answers! Hope that helps.
Hi, I and both of my daughters are diagnosed with hEDS. I had brain surgery for a double (heart-shaped) aneurysm. My sister was diagnosed with an aneurysm at the same time. I am told that hEDS does not cause aneurysm but i’m questioning that.
Can you please let me know if there is a way to stop the myoclonic jerks as my daughter is really suffering when it happens…always at night and randomly. I would really appreciate your help!
Hi Lin, so glad your surgery was successful! I am increasingly convinced from my observations of the large support groups online (20,000 + people) that aneurysms are common in all types of EDS, not just vascular, for which it is best known. That said, I’m not sure who diagnosed you or how, but maybe check out this post to see if they properly helped you rule out the vascular type:
http://ohtwist.com/about-eds/diagnosing-eds
And yeah, don’t you just love those myoclonic jerks? Not! I had them badly as a child – I thought I was “falling” in a dream when they happened. As my parents were sort of absentee, we never looked into this. I just lived with it and got on with life. Mine have reduced, but I”m not sure why and I”m not sure exactly what causes them. I will say that I suspect either low magnesium contributes, and/or it may have to do with head/neck position and how “loose” your spine is. I sometimes feel like it’s when I relax just enough for some bones to settle as I’m falling asleep that it happens. So again, I”m not sure if it’s neurological (harder to fix) or biochemical (easier to fix if you can find a supplement you tolerate). Hope that helps, you have my sympathy!
I believe that dysautonomia is present in many conditions and that it is the common link of many misunderstood and underdiagnosed disabilities. I realize you did tag autism in quite a few tags but didn’t make a significant mention. Dysautonomia, though only mentioned as hereditary in familial dysautonomia should really be thought as a genetic component of many spectrum disorders. There are many ties to the prevalence of autoimmunity in autism and fibromyalgia patients and though there are no funded studies it should be verified beyond reasonable doubt. Many genetic predispositions including eds seem to have overlapping conditions that would suggest heredity and autoimmunity. Thanks for this post. I was misdiagnosed since childhood with allergies and sinusitis though I had dermatographia, cyst formations, passing out frequently, and swan necking fingers. It wasn’t until I had 3 children on the autism spectrum of different degrees of severity that I realized many of their “autistic tendencies” came from me and can be contributed to dysautonomia.
I quite agree: I think dysautonomia is a symptom constellation, or result of other conditions/issues in the body, of which there are many lending to it, includinjg Lyme and more. I wrote about a few of the most common in the hypermobile community here:
http://ohtwist.com/wherefor-art-thou-dysautonomia
And you seem to be circling the same hill or elephant I am here also: http://ohtwist.com/the-chronic-constellation
Great minds think – and connect dots – alike! Cheers – Jan
I have nearly all of these but am having trouble getting a diagnosis! And it’s getting worse. Any advice? Thank you!
This is a tough question, as it sort of depends what area you are in, and what doctors you have access to. If you can find a GP or PCP who is just willing to even consider a diagnosis of either HSD or a form of EDS at a minimum, then I wouild point them to the EDS Toolkit for doctors we produced in 2018 here:
http://rcgp.org.uk/eds
It is by doctors (and some expert patients) and for doctors, and free to all. Otherwise, I strongly suggest finding and joining the nearest local support group to ask about the best doctors to see in your area. I would check out this website to that end:
http://chronicpainpartners.com
I’m sorry it’s so darn hard. Remember, almost no doctors have yet heard of the new diagnostic category that is sort of “invisible beneath the water line” to them that was newly recognized in 2017 called the Hypermobility Spectrum Disorders. So if you get a lot of pushback for considering EDS, try telling them about that, here:
http://ohtwist.com/hypermobility-spectrum-disorders
Good luck! And don’t give up! It’s taken some of us 25 years or more to get diagnosed. Most of our parents never were. We’re slowly bringing these conditions into focus for doctors.
I have most of these symptoms. I have Aortic dilation, flat feet, hypertension and pots, PVCs, anxiety disorder, secondary Sjögren’s syndrome, positive rf factor, low vitamin D, have had SIBO, have CVID because of Low IGA, have muscle weakness and pain in joints. Ankles roll and hurt when I walk, left hip pops out of place at times, I walk like out of Balance at times, have been to PT numerous times for shoulder and hip and leg/feet problems. Sometimes muscles are strong sometimes I’m so weak I can’t hardly carry a gallon of milk. I can fold my ears in half, they are very small ears with small ear lobes, have high palette in mouth. I get chest pain frequently and end up in hospital with high blood pressure. Have weird reactions to meds one time it affects me one way and another time like it’s too strong. I have an umbilical hernia, liver hemangioma, polyp on gallbladder. Recently started having throat problems. I had several times where I started gasping for air for no reason. So they are doing studies on my throat and rechecking umbilical hernia and gallbladder polyp. I’m supposed to have genetic testing in July at Baylor adult Genetic clinic. I have IBS-d and have always had constipation with bad cramps then diarrhea especially after eating pizza. I also have sleep apnea but can’t tolerate cpap because it feels like it’s chocking me which I think is because of fragile throat and central apnea’s that occur so I use a elevated head of bed with adjustable base to alleviate the snoring. I’ve also always had a deviated septum that causes me to breathe more out of one nostril than another.
Wow, yup, you definitely sound like a fellow hypermobile zebra! I’m glad you’ll be seeing a geneticist. Try to gather as much family history as you can (even if you think it’s unrelated – you might be surprised) to help them form as complete a picture as possible. Several CTD’s overlap a lot and need to be differentiated from each other.
I would also rule out celiac disease based on your reaction to eating pizza (gluten and dairy). You may test negative due to your selective IgA deficiency. (Celiac is IgA mediated reaction.) But you may also/still have IgG reaction too. (I do.) I would consider cutting out gluten and dairy if you can then. (Diarrhea is a strong sign of this.)
Sleep apnea is a tough situation for all the reasons you described. I’m glad you’ve found a workable solution for sleeping! I’m just now going down this rabbit hole at 52. (Just started to wake myself up snoring for the first time in my life. Had CNS apnea back in 2012 that simply eased up with increased Vitamin C and magnesium supplementation and time – about six months.) Make sure they check for cranio-cervical settling, Tethered cord and Chiari malformation with those symptoms too.
Best of luck to you!
I have so many of these symptoms. Just last year I dislocated my left knee and while still in a brace I dislocated the right knee and months later dislocated my elbow. I have dis located each knee about 12 times in 16yrs. While going to therapy for my knees the therapist said I have very loose joints. He would say oh your going to be so sore tomorrow and not once was I sore. He said I’m just an odd case . They would put the electrodes on to work my muscles in my leg and every time had a hard time getting it in the correct place. He said it’s like they move to a different place. Anyway I have so many more temperature regulation, migraines, thyroid, skin problems maybe elastosis perforans serpiginosa, arthritis, spondylosis ect. My dermatologist is sending me to a immunologist. Is thsi a good type of doctor to see for a problem like this?
Boy, good question! That’s the first I’ve heard of this “elastosis perforans serpiginosa”. And when I started to read about it, I couldn’t help thinking “this has to come with connective tissue disorders”. And yup! Sure enough it does as per:
https://www.aocd.org/page/ElastosisPerforans
I think it would be good for you to see an immunologist in general, yes, but especially if the allergist is sending you. We can have so many issues with our immune systems, from over-active mast cells (MCAS), to allergies, atopy, and all manner of skin and gut issues.
I hope you also get to see a shrewd (meaning EDS savvy) neurologist at some point too. But one thing at a time.
Best of luck to you!
Only just on my hypermobility diagnosis path, having already been diagnosed with chronic fatigue/ME, fibromyalgia, chronic pain, vocal cord dysfunction, pelvic floor dysfunction and hypertonicity, sleep apnoea, multiple food and chemical sensitivities, allergies, allergic rhinitis, and most recently either lipoedema, Dercum’s Disease or both. I think it’s Dr Karen Herbst with the tissues issues quote.
Oh interesting, and welcome Catherine. I’ll have to ask one of Dr. Herbst’s patient’s about that. I know that Dr. Heidi Collins was quoting whoever it was in the title of her 2014 EDNF talk – she said so herself in the talk. Anyway, sorry you “enjoy” all these issues with your tissues… my best friend has Stage IV lipolymphedema and is fighting for her life. (She’s starting to finally tilt the tables back in her favor yay. Her story: http://morethanfat.com) I hope you are getting good support, diagnosed or not. Good luck. And keep the EDS Toolkit for doctors handy for yours:
http://rcgp.org.uk/eds
I think I can tick at least half a dozen of these just by what I know. I could probably tick off more if I knew for sure that they are my symptoms as some you’d probs have to be told by a doctor that you have. It may not be much but I reckon I’m probably somewhere on the hsd. If only I can get a doctor to clarify this and help treat it. I was told ages ago I had hypermobility and struggled for a while as things got worse and then last yr I got told there’s nothing wrong with me, just have low core and exercise will help fix it. This three me off to much and made me feel like a fake. But I’m ready to fight for my diagnosis
Good! Trust your gut, and do fight for your diagnosis. Though try to use honey, not vinegar – most doctors have not yet even heard of the new diagnostic category of the Hypermobility Spectrum Disorders, and still only remember the grossest signs of the rarest types of EDS. So appeal to their curiosity, and arm them with the latest info via the EDS Toolkit here:
http://rcgp.org.uk/eds
The above is sort of a Cliff notes of it all by and for doctors. And if that’s too hard to share (because you can’t print it out exactly, just share the link which may be hard to remember), then feel free to poin them to my site which has a page of resources including that just for doctors here:
http://ohtwist.com/about-eds/for-doctors
And do yourself a favor, and make a table (aka a spreadsheet on computers) of your family history as best you can. list ALL the issues and symptoms your family has had on the left side in the first column. This may be a really long list. That’s okay. Then list the names of your mom and dad and siblings across the top, and maybe aunts and uncles. I would do one table for each “side” of the family. (E.g. mom’s side, vs dad’s side) if able. (I only had my dad’s side to go from when I did this. I now have a cousin diagnosed on my mom’s side too.) Anyway, then start checking off the boxes under each name beside each issues/symptoms/sign and watch a clear pattern emerge showing which among you are the most affected. Again, list everything, even if you think it is unrelated – let the doctor(s) decide what it may point to. Trust me, they’ll thank you! Good luck.
I am nearly in tears! First, I have all but 3 or 4 of the symptoms listed here. Some of the rarer ones, such as Gorlin sign, 3 of 4 of my kids and several distant cousins have. Most of these I’ve had since early childhood. I was told that I was lazy, oversensitive, a hypochondriac, and much more. I was diagnosed with Fibromyalgia at age 46. Even then, many doctors were unsure because of the things that aren’t typical of fibromyalgia. Seeing this information at nearly 58 has made me feel like I’m not alone, I’m not crazy, I’m not a freak. THANK YOU!!!
You’re quite welcome! This is exactly why I wrote this page… to sort of bait the hook for folks like yourself. Of course, we can’t say for sure this is what you have (just to be pedantic) but… I highly suspect so with you. And we still have to determine what form.
But, you now have a lead, and hopefully will find a doctor who will follow it. I highly recommend the EDS Toolkit for Doctors I helped co-author here for any you find who are willing to consider this:
http://rcgp.org.uk/eds
Cheers!
I have almost all of these symptoms. I am tired of doctors blowing me off. I am just going to focus on wellness. Do you have an article of a recommended supplement regimen? That would be super useful!
I so feel you and get it! Alas, no single supplement regimen works for all but… the best I can point you to for now is the Cusack Protocol, by Deborah Cusack. Her blog talks about her success but doesn’t share the “recipe”. You can get that from her in her Facebook group if you’re willing to use that platform. Just look for “Cusack Protocol” on Facebook and you’ll find it/her.
https://ouredsjourney.weebly.com/
I personally recommend high dose vitamin C and magnesium, as my geneticist first recommended. And I just remembered I have a subsection or two on my EDS Resources page covering both Recovery Stories and Nutrition here (scroll way down, sorry – it’s loaded):
https://ohtwist.com/eds-resources
HTH! (I’ve done best with high dose C and mag and potassium myself.) But always start low and slow, and only one thing at a time.
And… I would try to consult a naturopath if you can. Regardless of dx. They take a functional medicine approach that can really help us.
Thank you so much. I looked into the Cusack protocol and am trying it. I’m currently on culturelle and pqq as I’m taking it low and slow and only adding one drug at a time. I would have never known about this if I didn’t ask you! Thank you!
Ah, glad to hear, and you’re quite welcome! Yes, take it one supp at a time, go low and slow until you know how you tolerate each one. (And be sure to update your doctor too to watch for any drug interactions/contraindications – rare, but they exist.) And good luck!
I have so many of these. When I was 40 (I am 47 now), I went to my doctor to complain of rather sudden onset of all over joint pain. He basically told me I was fat and that was my problem. I didn’t go back to a doctor for a while after that. When I did go to a new doctor, she has tried to figure out what is going on, but hasn’t come up with anything really. I have calcific tendinitis in every joint they’ve x-rayed so far (both shoulders, both elbows, one thumb, I stopped asking after that) and osteoarthritis in all of the same. I was sent to a rheumatologist once, in 2015, who gave me the same answer, “I don’t see an inflammatory process, you’re just overweight”. I even asked him if it was normal or typical for a 40 year old otherwise healthy female to suddenly develop osteoarthritis in all of her joints at the same time, he just sort of shrugged and didn’t answer me. I have an appointment with a new rheumatologist in July. Fingers crossed I can figure something out.
Oh my word if I had $10 for every time a doctor said “you’re just overweight” I’d be rich!! I’m so sorry for all that dismissal. But way to stick to be a poodle on the pantleg of the problem. Trust your gut – always. And persist. I hope this new rheumy does better by you. You might send them the EDS TOolkit for doctors to study if willing, it’s sort of a Cliff Notes for the condition:
https://rcgp.org.uk/eds
And no, that’s not “normal”. Unless you’re hypermobile. When our joints may suddenly all start hurting a lot more or going out almost at once due to hormonal fluctuations. IOW, you’re not losing your mind, just your body… and just temporarily. (I’m back walking again after my onset “cascade” at 45 eight years ago.) Good luck!
I have most of these symptoms on this list but the most surprising thing is the EMF disturbance. This probably sounds crazy to anyone who doesn’t experience it but I “break” machines. For example, cash registers malfunction when I’m in line, batteries drain, light bulbs blow out, radio/ tv gets staticky, WiFi interruptions, vehicle break downs, phones spazzing out… and the list goes on. I never once thought it could be connected but it makes sense to me. Every thing wrong with me is connected and it’s funny to me that the cause is connective tissue.
I totally believe you! While uncommon in the “normal” population, it is not all that uncommon in the hypermobile cfommunity I’ve found. I also “blow” some elecftronics – not quite that often/badly, but uhm, I once took out the whole engineering department at the City of Milwaukie because I carry a “charge”, ahem. (I consigned myself to desk duty only after that, my boss didn’t disagree.)
Love the analogy – connectivity issues with connective tissues 😉
Wow. I have the top5 and 50 others. I have always thought my issues were connected even from the beginning when I considered there must be a common systemic cause for both my digestive issues and chronic pain. Then when they both flared at the same time (female hormonal changes – and people in my GP group can relate). I was certain.
I wish that doctors could get on board with seeing all of you.
I also wanted to mention that like another person I have tons of cysts. In addition to the ganglion cysts in my wrists, hip and feet, I also have cysts in my ovaries (not PCOS) and fibrocystic breast condition.
Way to trust – and heal and heed – your gut, Amanda! Welcome to the large and growing pool of people with systemic connective tissue issues that doctors rarely recognize, sigh. This is why I’m blogging and tweeting – steadily pounding the drum – to slowly bring people along, both doctors and patients, one by one.
Not all of us will have EDS/HSD – some will find they have a very similar or related CTD like Marfan Syndrome, or Stickler Syndrome, or Loeys-Dietz, etc. But the issues are all quite similar, with some isolated stand-out differences or “sign-post” symptoms – e.g. arterial tortuosity in LDS, clubfoot at birth in vEDS, brittle bones in OI, etc. But the vast majority of our issues overlap, since the body can only express itself in so many ways, right? Thanks for chiming in!
Wow! I can tick yes to about 45 of these.
I was super flexible, but accident prone. I was told I was double jointed, but not warned of any risks of doing ballet, gymnastics or showing off my crazy joints. I was sick a lot, I have food & chemical sensitivities, I have had anxiety since I was 5 or 6, although it was called being nervous & a nervous stomach back in the 70’s. Unexplained nose bleeds. Arthritis started in my knees in my teens & by 18 had to give up my dreams of a being a ballet dancer due to so many knee & ankle injuries. Always covered in bruises, because the slighted bump caused them.. Can’t wear contact lenses & have a weird astigmatism. Unexplained pain, chronic fatigue, intermittent Reynards, rheumatoid arthritis & fibromyalgia.
All the years of being called a malingerer.
My step daughter discovered a study on hypermobility & anxiety yesterday & suddenly I am down this rabbit hole. Maybe at 54, I finally know it was all related.
Yup! You definitely sound like one of us! I’m so glad she found that study, and you’ve fallen down the rabbit hole with my site’s help. Some wise anonymous (uknown) person once quipped: “If you can’t connect the issues, think connective tissues.” I so wish I knew who it was to give proper credit. (It was not Dr. Heidi Collins, she states up front she just quoted them herself in her 2014 talk of the same name.) Anyway, if only medicine wouldn’t silo the body so much, and stop calling this rare, more doctors would see it. I recommend sharing the EDS Toolkit for doctors with any you have that seem sympa to that end here: https://rcgp.org.uk/eds
Good luck! And think marathon not sprint.
Is that what EMF disturbance is? I went through 5 Swatch watch’s, in the 80’s before that wouldn’t replace them anymore & I had to change watch batteries everyone month or so. I eventually gave up wearing a watch.
I had sort of forgotten about that, but I can’t keep my phone in pocket or I drain the battery quicker & I’m lucky to get home after a work day before having to recharge my Apple Watch. I also don’t ‘activate’ some automatic doors. I used to have to wait for someone to come along to get in or out my local supermarket, because the door sensor did not recognise me.
Yes, everybody’s experience is different. But some of us will sort of “drain” batteries faster, and blow various electronics and light bulbs even from a distance. (I have a crazy story about my friend David’s ex-girlfriend blowing the lights on one of our city bridges on the regular… he was as skeptical as anyone, until he literally saw it happen in action.) It’s weird that you can’t activate the automatic doors – that’s a first! But I completely believe you.
I took out the entire engineering department at the City of Milwaukie one night in 2010 just trying to add memory sticks to 3 computers there to help buy time until the main tech refresh could happen. First time, thought it was a fluke. Second machine – uhm, okay, weird coincidence! Third machine – I’m outta here, and don’t ever send me out to touch the machines again lol! (I was a temp admin help in the department but had the skills to do some light tech fixes like this.) You’ve definitely found your people.
I only have 22 of these symptoms. What’s my likelihood of having this? Should I put money into trying to diagnose it? I do have a lot of joint problems…
Well, that’s a tough call as I don’t know you personally/haven’t seen you, nor am a doctor. But… yes, with even that many from the list (whichever ones, doesn’t matter) and your history of joint problems? Yes, I strongly suspect you of some kind of connective tissue disorder. (EDS, HSD, Marfans, etc.)
Whether to pursue a dx? That’s another tough call… I always encourage folks to try if willing and able, as otherwise we keep maintaining medicine’s false narrative and confirmation bias that “EDS is rare”, when in fact, the collection as a whole (including hEDS) is far from rare. Truly. So the more who get diagnosed, the merrier. (At some point hopefully in my lifetime, the medical gatekeepers will finally agree.)
In any case, if you have the energy and can swing it, yes, go for it. I highly recommend tapping the EDS Toolkit for Doctors (I helped co-author) to that end: https://rcgp.org.uk/eds (anyone can use this worldwide, it just happens to have been generated in London and is hosted by the NHS.) Just think marathon, not sprint. And don’t be discouraged if you get batted down right out of the gate initially, especially by rheumatology. Doctors have only been told about and/or can only remember the grossest signs of the rarest types, so tend to dismiss anyone who can still walk and talk unaided. (Whence this blog – I had to go from walking to wheelchair in 3 weeks in Janauary 2012 before finally being believed and diagnosed with anything besides “depression” at 45.)
Also, gather your family history as I recommend here to help make your case if you can: https://ohtwist.com/about-eds/diagnosing-eds
Hope that helps, good luck!
Oh my goodness! I am 49 years old, and was finally diagnosed with hEDS a year ago. I am only missing 7 of these symptoms/comorbidities! My two daughters also have at least half of these already, and they’re only in their early twenties. This is such a devastating disease. Every part of my body is hurting, malformed, or malfunctioning. I feel so sad for all of us.
So sorry you are beset by this painful systemic body wide condition too Summer. But so glad you got diagnosed last year at least! So few still do. (Why I wrote this blog and have consulted on the EDS Toolkit for Doctors hosted by the NHS.) This page in particular seems to help open people’s eyes as they tick off so many of the items like you said. To quote Dr. Afrin, who was trying to describe Occam’s Razor: do you really think there are 57 different things wrong with your patient, or might there be just one or two systemic conditions underlying so many problems that could explain them all? Yup.
(I also like Hickam’s Dictum: patients are entitled to as many diseases as they damn well please!) Yup! Welcome to the Great Clan Dumpty! You’re in good company!
Very interesting and helpful post. I was diagnosed with EDS at 11 after a period of multiple daily dislocations and subluxations. Now in my late 40s, I have all 5 from the top list and over 50 of the symptoms from the bottom list. I am the first in my family to be diagnosed but I could easily name 4 other members who probably have EDS as well. Sadly, I find that few doctors seem to put together the whole picture. Many even are so unfamiliar with EDS that they want to discount or ignore it completely. There are probably a whole lot of people who have never heard of EDS that are suffering needlessly. It really needs more publicity and doctors need better education about it.
Sorry to hear you share this lousy condition and were bad enough to be diagnosed so young. And completely agree about the need to keep raising awareness. I’ve found much the same – the few doctors that know about it have really off or outdated information, and others are in total denial as you said. It really sucks. I totally believe you about the 5 and 50. Like, we ARE the frequent flyers in their medical offices, hello!
That’s why I’m blogging and tweeting so hard. Which landed me as a co-author of the EDS Toolkit for doctors in 2018: https://gptoolkit.ehlers-danlos.org.
I’m also co-authoring a book on Autism and EDS now with several others. And, still trying to write my own. (The Goal posts keep moving as I keep collecting insight and diagnoses, but they’re slowing down a touch, finally.)
i read this blog it is so useful for me thank you
23 signs you grew up with ehlers-danlos syndrome
Don’t forget eagle syndrome, may thurner, nutcracker, MALS, smas
I have those on my “Common Comorbidities” page, smile. Thanks! Here:
https://ohtwist.com/about-eds/comorbidities
A couple more things to add to the list that my kids have gone through…
My son had Bell Clapper Deformity, where the connective tissues was not there hold his testicle to his sack.
My daughter, myself and my sister all had to have our hymens removed. The connective tissue was hyporesponsive to starting our periods. Couldn’t wear a tampon either.
Oh interesting, thank you for sharing! First I’ve heard of either of those things, but that’s what’s great about your comment: we can all learn. (And, nothing surprises me anymore where connective tissue disorders are concerned!)